Background on AML
To begin, let's learn something about AML.
Click the "next" button to proceed through each section.
Epidemiology
(data from National Cancer Institute and American Cancer Society)
- Estimated number of new cases in the US for 2010: 12,330
- Estimated number of deaths due to acute myeloid leukemia in the US for 2010: 8,950
- Adults > Children
- Average age at diagnosis 67
Next
Definition
- Clonal hematopoietic stem cell disorder usually originating in the marrow
- Characterized by a proliferation of immature myeloid cells (blasts or blast equivalents) and typically, a block in maturation
- Blasts or equivalents comprise >20% of cells in marrow or blood, or specific AML-defining genetic abnormalities
- Many subtypes recognized based on distinct features and/or differences in prognosis
Back Next
2016 WHO classification of AML
- AML with recurrent genetic abnormalities
- AML with t(8;21)(q22;q22); RUNX1/RUNX1T1
- AML with inv(16)(p13q22) or t(16;16)(p13;q22); CBFbeta/MYH11
- APL with t(15;17)(q22;12); PML/RARalpha
- AML with t(9;11)(p21.3q23.3); MLLT3-KMT2A
- AML with t(6;9)(p23q34); DEK-NUP214
- AML with inv(3)(q21q26.2) or t(3;3)(q21;q26.2); GATA2, MECOM
- AML (megakaryoblastic) with t(1;22)(p13q13); RBM15-MKL1
- * AML with BCR-ABL1
- AML with mutated NPM1
- AML with biallelic mutations of CEBPA
- * AML with mutated RUNX1
Back Next
- AML with myelodysplasia related changes
- Therapy related myeloid neoplasms
- AML not otherwise categorized
- AML minimally differentiated
- AML without maturation
- AML with maturation
- Acute myelomonocytic leukemia
- Acute monoblastic / monocytic leukemia
- Pure erythroid leukemia
- Acute megakaryoblastic leukemia
- Acute basophilic leukemia
- Acute panmyelosis with myelofibrosis
- Myeloid sarcoma
Tools for Diagnosis
Morphology
- Enumerate blasts
- Need >20% myeloid blasts in the blood or marrow to establish a diagnosis of AML using WHO criteria
- Suggest lineage
- Auer rods are the only lineage defining feature
- Myeloid blasts
- Larger, more cytoplasm, granules
- Lymphoid blasts
- Smaller, less cytoplasm, granules are rare
- Other blast equivalents may be recognized by morphology
- Abnormal promyelocytes, monoblasts, promonocytes
Back Next
Cytochemistry
Flow Cytometry
Genetics
- Many genetic changes have been described in AML which have prognostic significance
- Cytogenetic changes
- Several are included under the WHO category AML with recurrent genetic abnormalities
- Some of these have flow cytometric correlates
- Gene mutations
- Include FLT3 ITD, NPM-1, CEBPa
- All have prognostic significance
- Some are included as provisional entities in the WHO classification
- Some flow cytometric correlates have been described
Back
Continue
Case Introduction
- The following case example will be used to illustrate the application of flow cytometry in the diagnosis of AML.
- As you work through the case, you will be asked questions about key points.
- Give it your best guess, and learn from the response. These case-based questions will not be graded.
- Your knowledge will be tested/graded at the end of the e-learning activity.
Continue
Clinical History
- A 29 year-old pregnant female (G3P1A1) presented at ~6 weeks gestation with night sweats and nausea for one week.
- She had also experienced an episode of gum bleeding while brushing her teeth approximately one week prior.
- She was found to have leukocytosis, anemia and thrombocytopenia on routine CBC:

- Peripheral blood smear review showed blasts.
Continue
Flow Cytometry
- A peripheral blood specimen was received in the flow cytometry lab.
- Four color flow cytometry was performed using a BD FACSCalibur™ flow cytometer.
- Ungated, cluster analysis was performed with BD Paint-a-Gate™ software.
- FCS files in FCS2.0 format are also available for download and analysis in your own lab.
- Antibody tubes with the following antibody combinations are included for review.
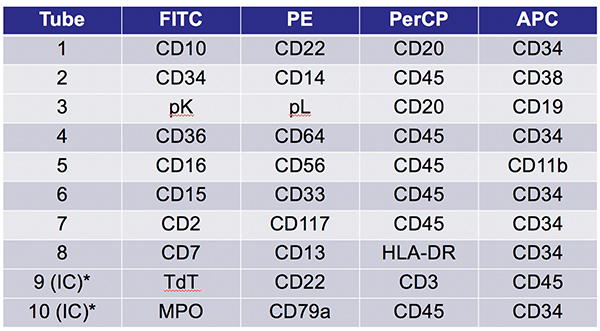
*Intracellular tube
Which antibody combination would you use to identify blasts?
Click on a tube to see if you’re correct:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Continue
Blast Identification Summary
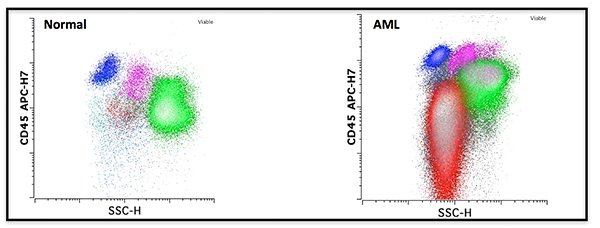
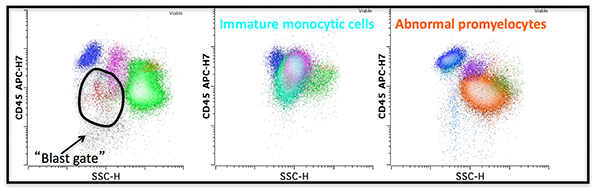
- Acute leukemias are often first recognized on a CD45 versus SSC plot.
- CD45 versus SSC allows one to generate a rough 4 part differential.
- Lymphocytes, monocytes, myeloid forms, and “blast” area (dim CD45 and low SSC).
- Lymphocytes, monocytes, myeloid forms, and “blast” area (dim CD45 and low SSC).
- Most blasts have decreased CD45 expression.
- However, cells present in the “blast gate” are not all blasts.
- Basophils, plasmacytoid dendritic cells (PDC), hypogranular myeloid cells, early monocytic cells.
- Basophils, plasmacytoid dendritic cells (PDC), hypogranular myeloid cells, early monocytic cells.
- Therefore, specific markers of blasts are required for definitive identification of blasts (usually CD34 and CD117).
- Additionally, markers are required to differentiate blasts from cells that may be contaminating the blast gate.
- Also of note, not all blast equivalents fall into a standard CD45 versus SSC blast gate.
- Immature monocytic cells
- monoblasts, promonocytes
- Abnormal promyelocytes
Continue
Blast Cell Gate Video
More information about the blast gate can be found in this video. You can access the full Blast Cell Gate video by logging into your ICCS account and selecting "Member Services".
Continue
Enumeration of Blasts
Question
INCORRECT: Please Try Again.
CORRECT
Discussion
- Blasts are identified based on expression of markers of immaturity (eg. CD34, CD117), light scatter properties (FSC/SSC) in combination with CD45 moderate expression (“Blast gate”), and other combinations of myeloid antigens.
- Blasts may be enumerated from any of the antibody tubes that contain identifying markers.
- However, several factors confound enumeration in the marrow.
- Hemodilution
- Artificially decreases the blast percentage
- Partial lysis of erythroid precursors
- Removes erythroid precursors from the denominator of the blast percentage artificially increasing the blast percentage
- Inclusion of blast equivalents
- Hemodilution
- Therefore, morphology is often regarded as the most reliable method (gold standard) for blast enumeration in the marrow.
Continue
Phenotype of Blasts
What is the phenotype of the blasts?
View plots from each of the tubes and make a list of the antigens expressed by the blasts. Then continue to see if you got the phenotype correct.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Continue
Summary of Phenotype
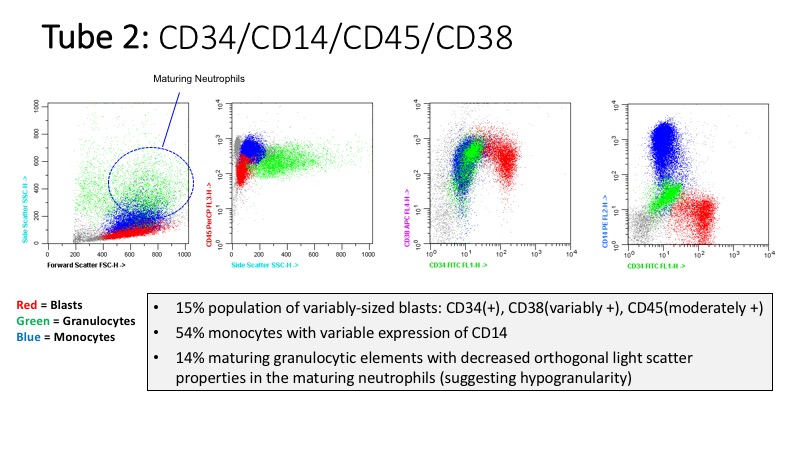
This case shows a 15% population of variably-sized blasts with the following immunophenotype:
CD34 (+)
CD2 (few +)
CD13 (+)
CD15 (partial +)
CD25 (few +)
CD36 (few +)
CD38 (variably +)
CD45 (moderately +)
CD64 (few +)
CD117 (+)
CD123 (variably +)
HLA-DR (variably +)
MPO (dim +)
TdT (-)
Other myeloid and lymphoid antigens pre-dominantly (-)
Question
CORRECT: Based on the presence of myeloid antigen expression (CD13, CD33), even in the absence of equivocal MPO.
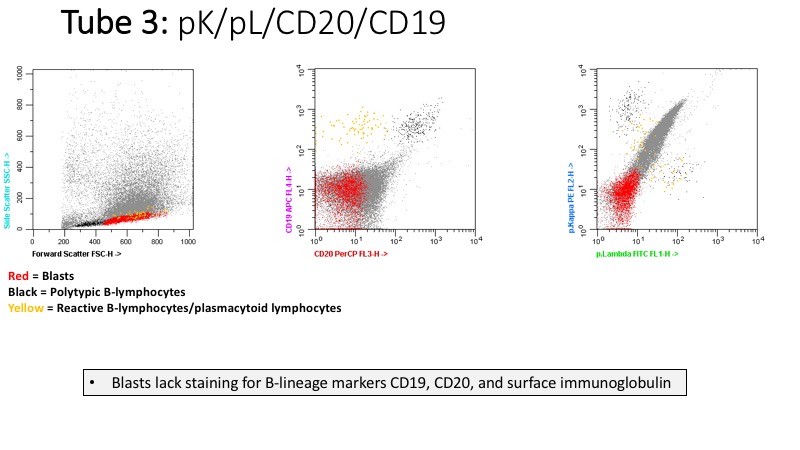
INCORRECT: There is no expression of B-lineage markers: CD19, CD20, CD22, CD79a.
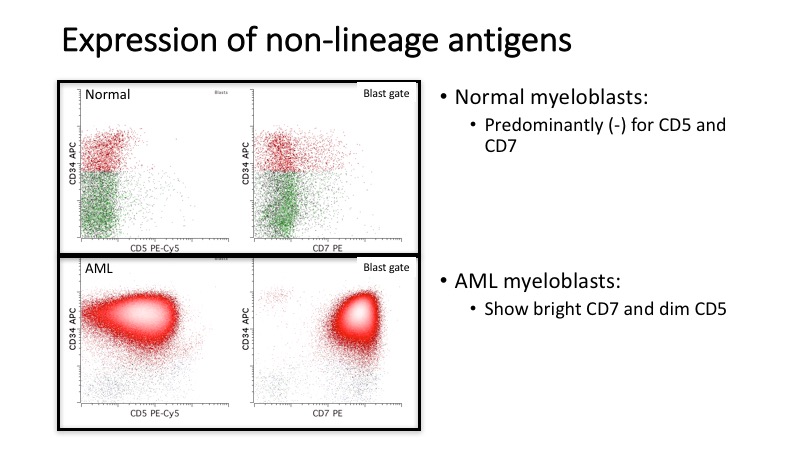
INCORRECT: There is no expression of T-lineage markers: surface or cytoplasmic CD3, CD4, CD5, CD7, CD8, CD1a.
INCORRECT: Are usually negative for CD34, CD117, and positive for CD36, CD64, CD11b, bright CD33.
Commonly Used Antigens for Flow Cytometric Evaluation of AML
Progenitor cell
|
Erythroid
|
Recommendations of Bethesda International Consensus Conference.
- Initial assessment of a new acute leukemia requires evaluation of myelomonocytic and lymphoid cells
- Myelomonocytic cells: CD7, CD11b, CD13, CD14, CD15, CD16, CD33, CD34, CD45, CD56, CD117, and HLA-DR
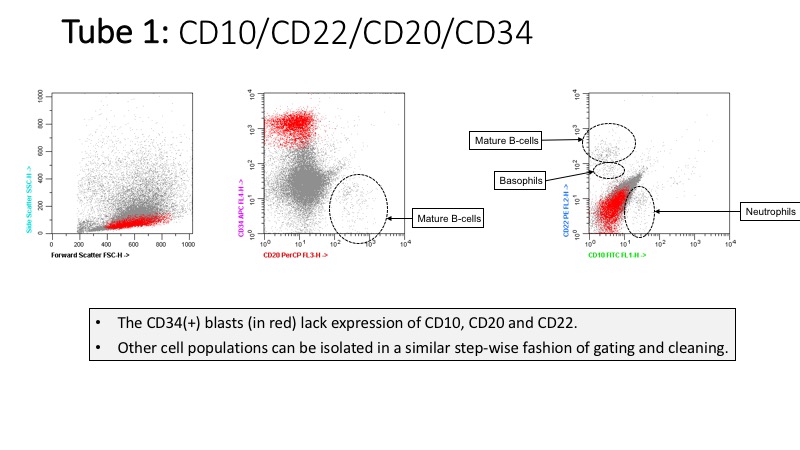
- B cells: CD5, CD10, CD19, CD20, CD45, kappa, and lambda
- T cells: CD2, CD3, CD4, CD5, CD7, CD8, CD45 and CD56
- Additional markers should be used on an as needed basis.
Question
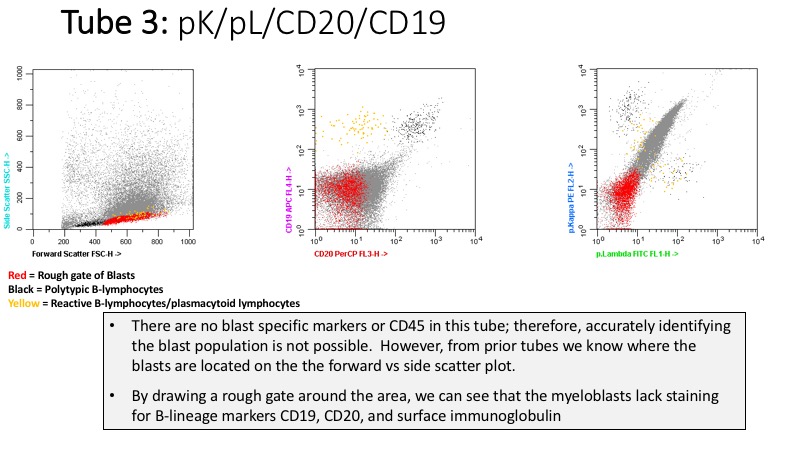
CORRECT: Is helpful in detecting immunophenotypic aberrancies in myeloblasts, such as partial CD22 or CD10 expression. There were no blast aberrancies present in this tube.
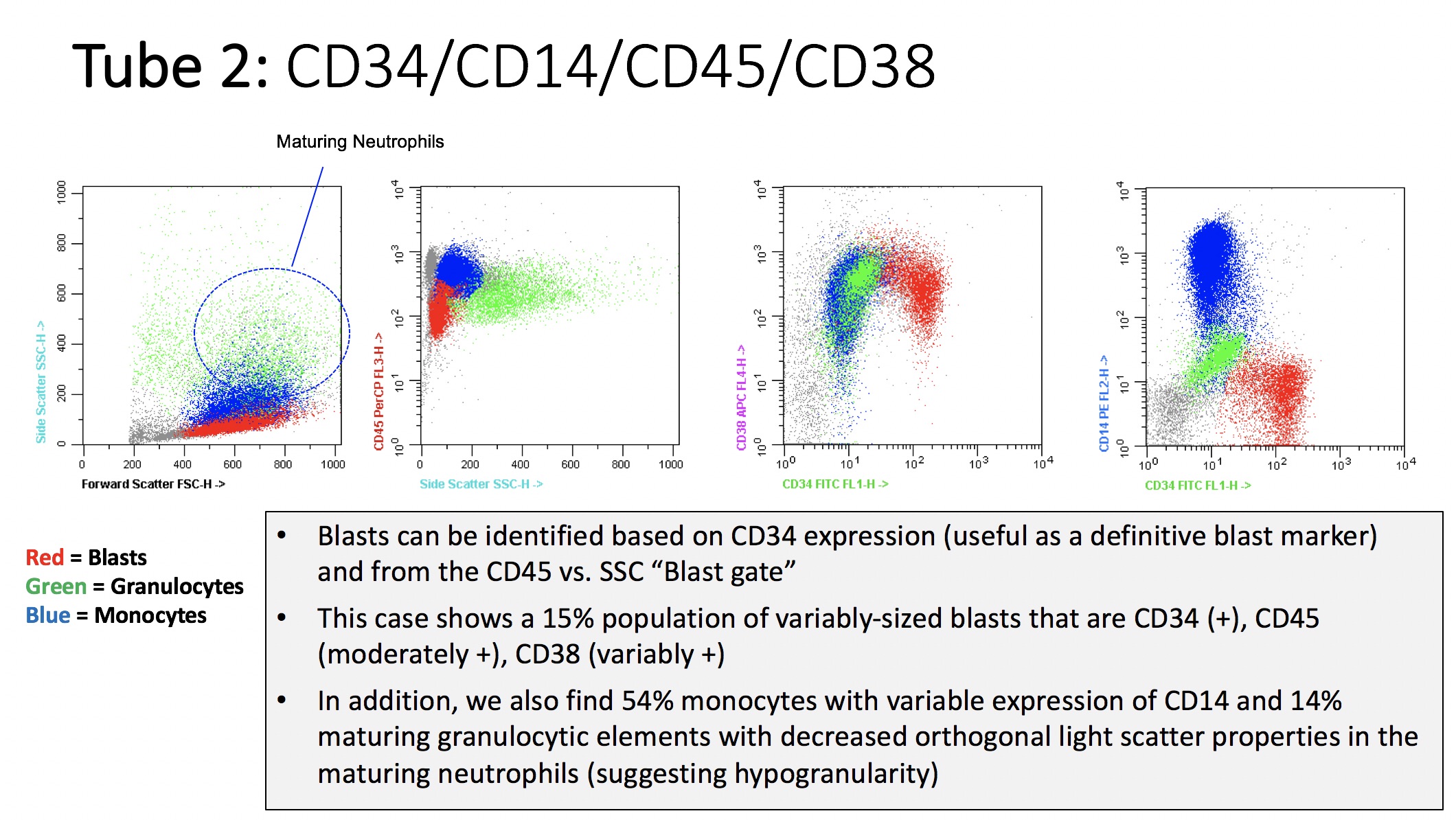
CORRECT: Is helpful in detecting immunophenotypic aberrancies in myeloblasts. CD38 is variably and slightly dim (+) on aberrant blasts in this case; however, the CD34/CD38 expression pattern appears relatively normal.
CORRECT: Is helpful in detecting immunophenotypic aberrancies (e.g., CD19 expression) in myeloblasts. There were no blast aberrancies present in this tube.
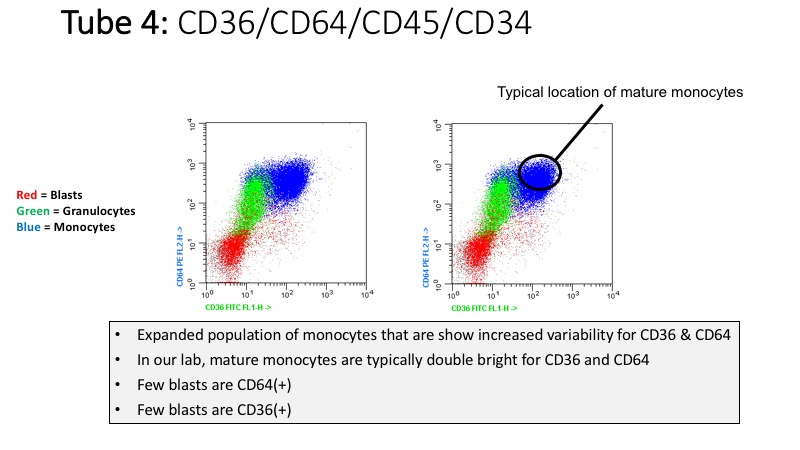
CORRECT: Is helpful in detecting immunophenotypic aberrancies in myeloblasts, such as CD36 and/or CD64 expression. Normal myeloblasts are negative for CD36 and CD64. There is a minor subset of CD36 and CD64 expression in aberrant blasts in this tube.
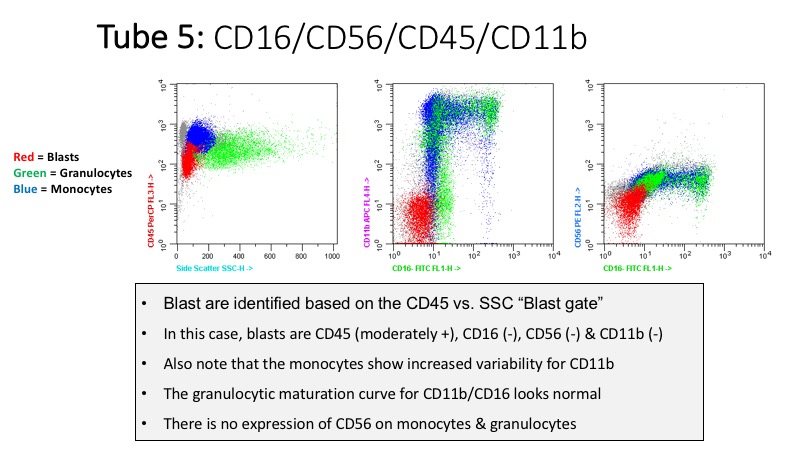
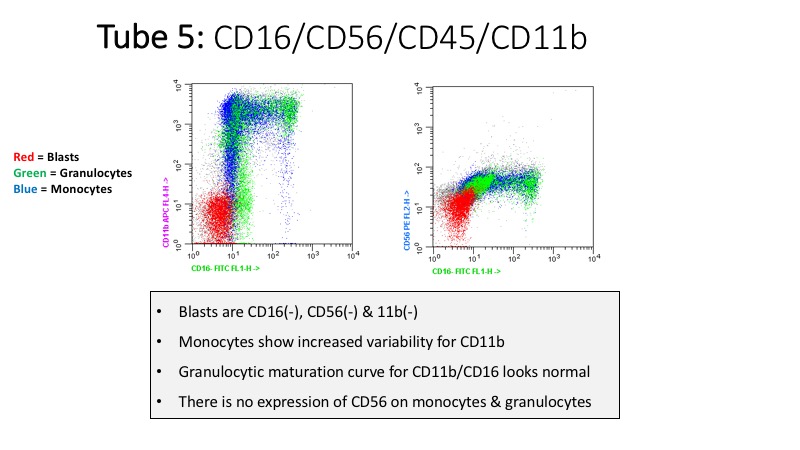
CORRECT: Is helpful in detecting immunophenotypic aberrancies in myeloblasts, such as CD56 and CD11b expression, CD45 bright (+) or CD45 (-). There were no blast aberrancies present in this tube.
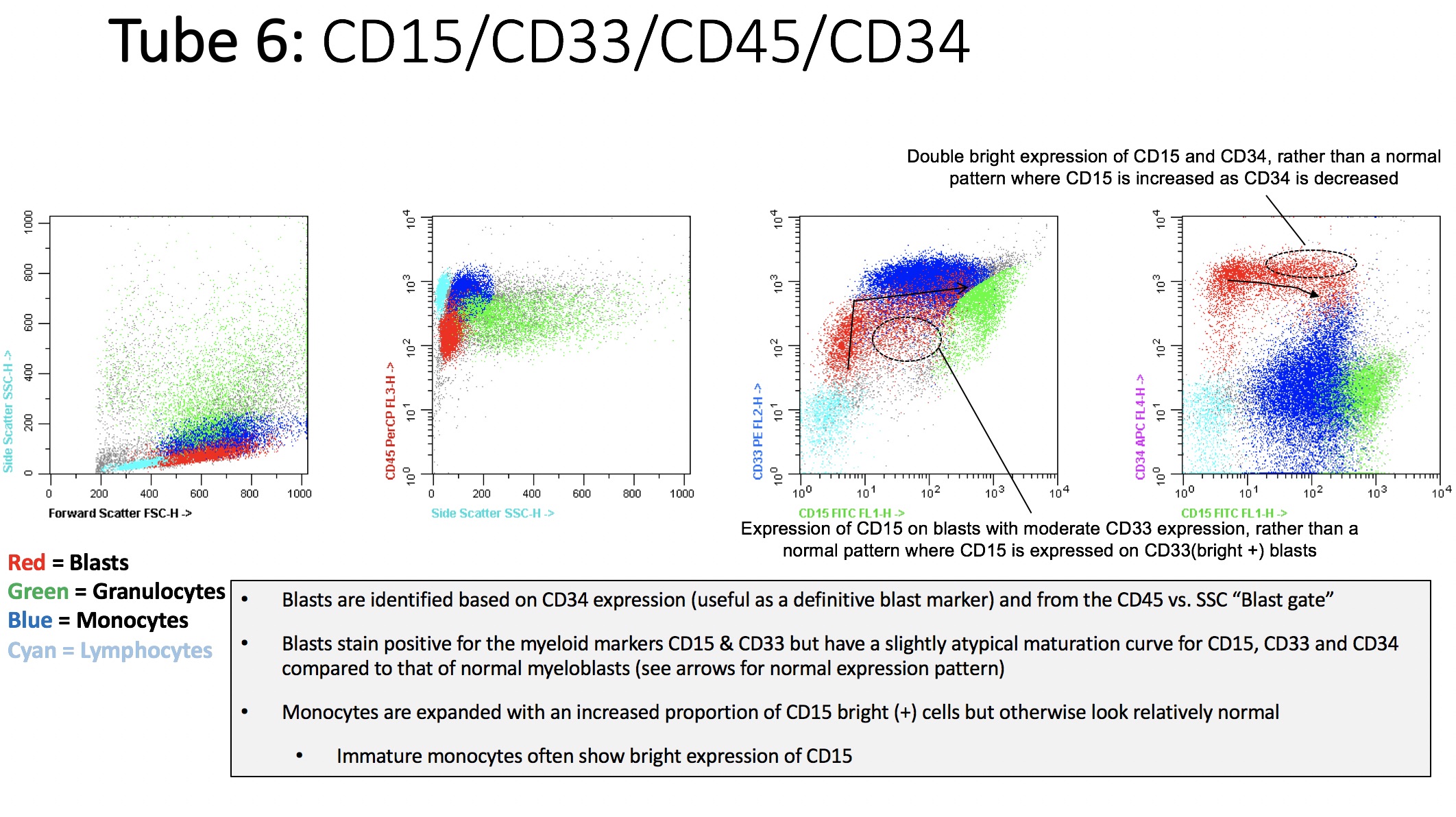
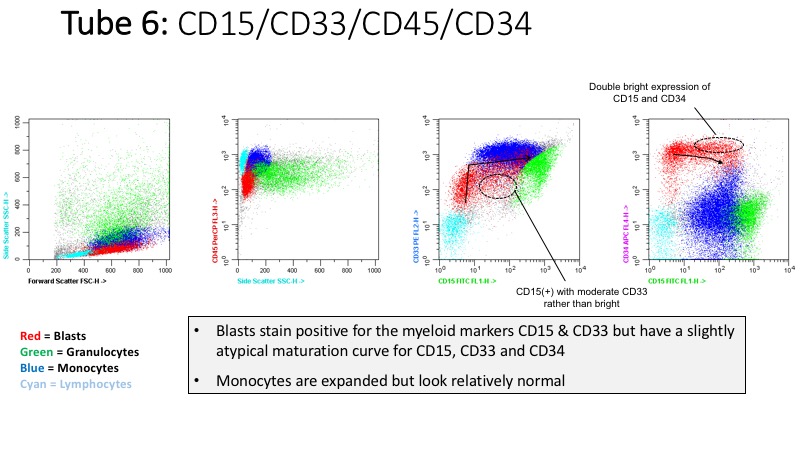
CORRECT: Is helpful in detecting immunophenotypic aberrancies in myeloblasts. In this tube, aberrant blasts show an abnormal expression pattern for CD15, CD34 and CD33.
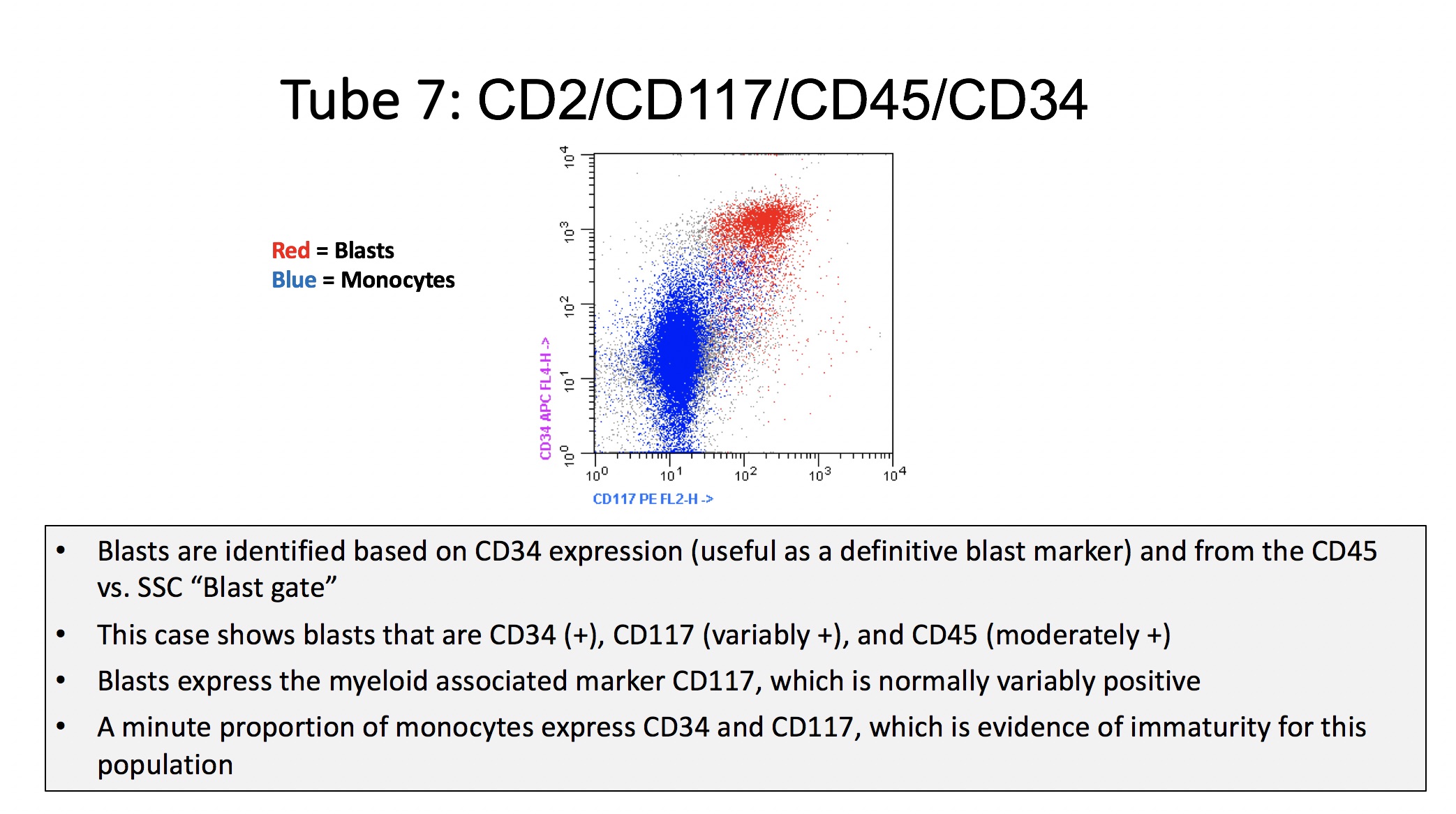
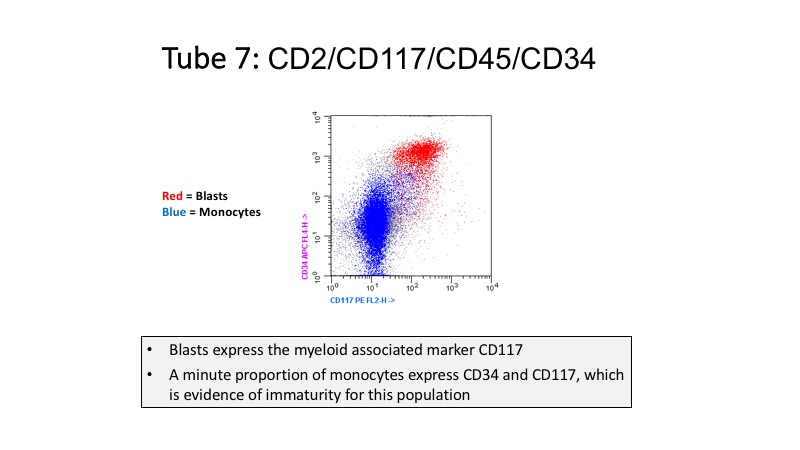
CORRECT: Is helpful in detecting immunophenotypic aberrancies in myeloblasts, such as CD2 expression, CD117 bright (+) or CD117(-). No blast aberrancies were present in this tube.
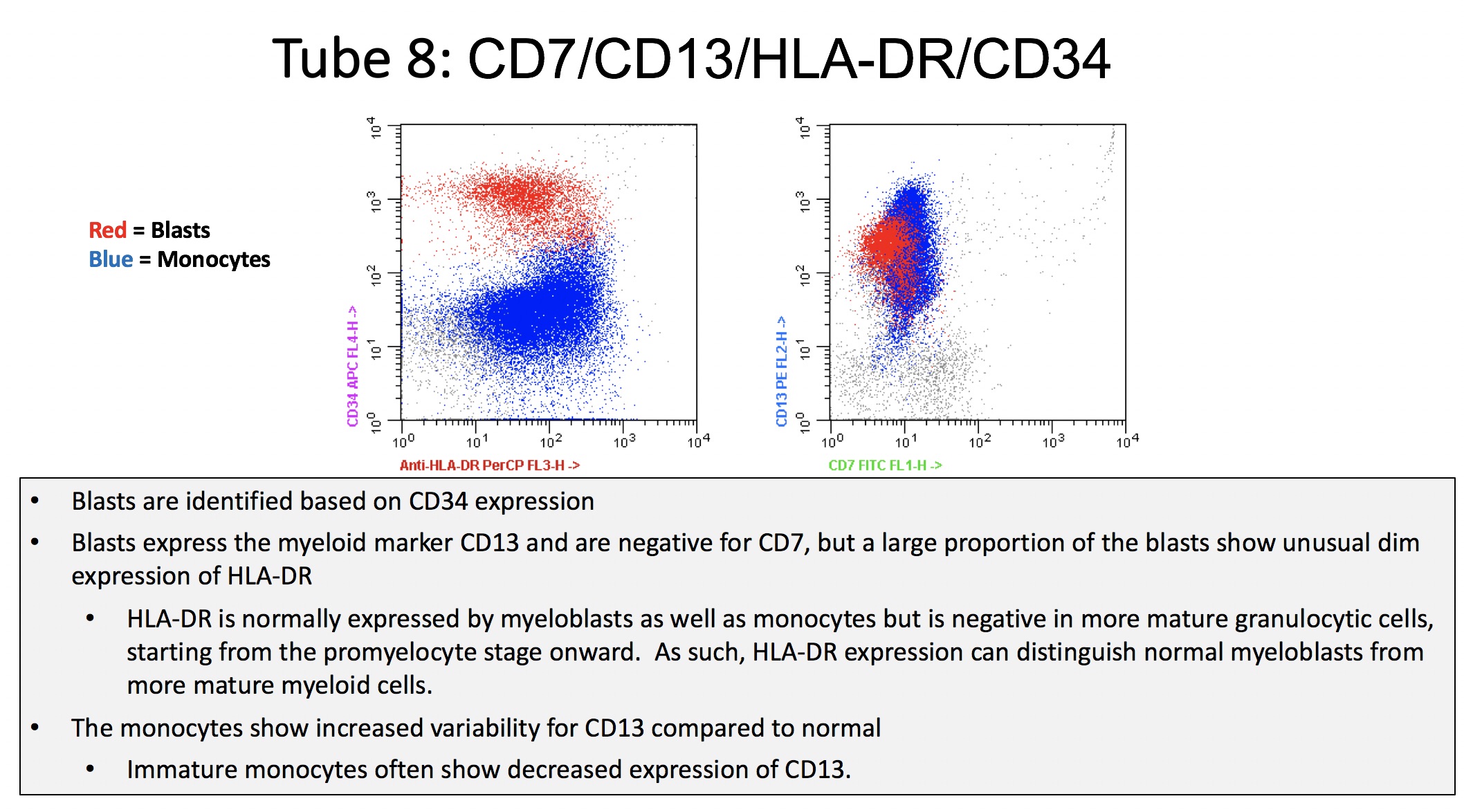
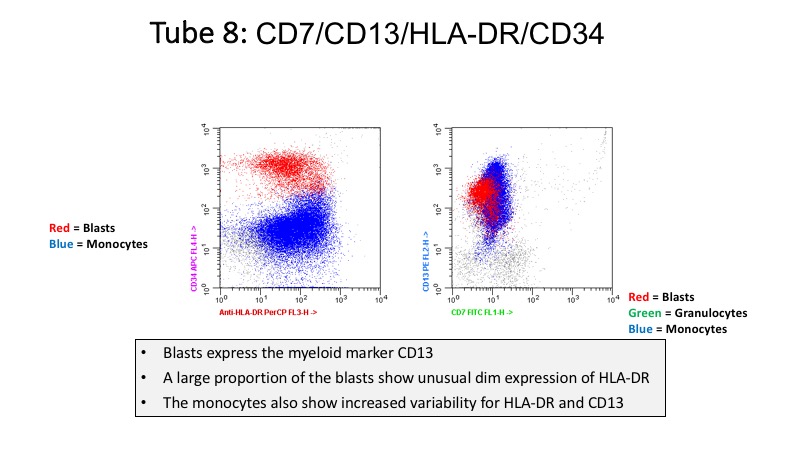
CORRECT: Is helpful in detecting immunophenotypic aberrancies in myeloblasts, such as CD7 expression, CD13 bright (+) or CD13(-), and HLA-DR dim (+) or (-). The blasts show slightly dim expression of HLA-DR in this tube.
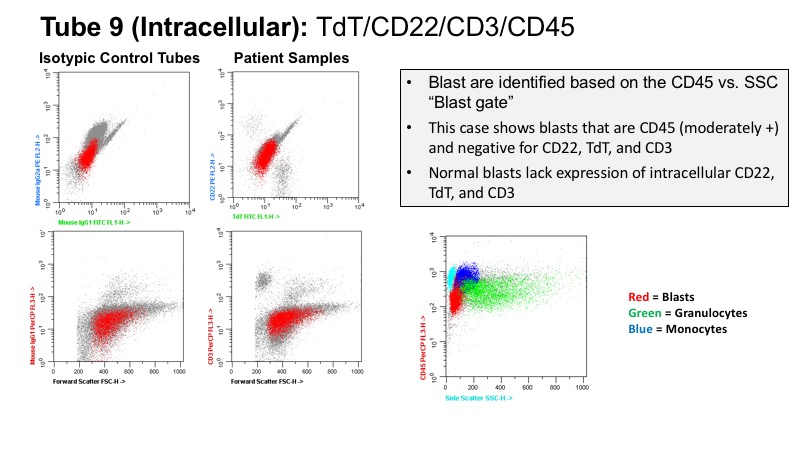
CORRECT: Is helpful in detecting immunophenotypic aberrancies in myeloblasts, such as expression of TdT, CD22, or CD3. There were no blast aberrancies present in this tube.
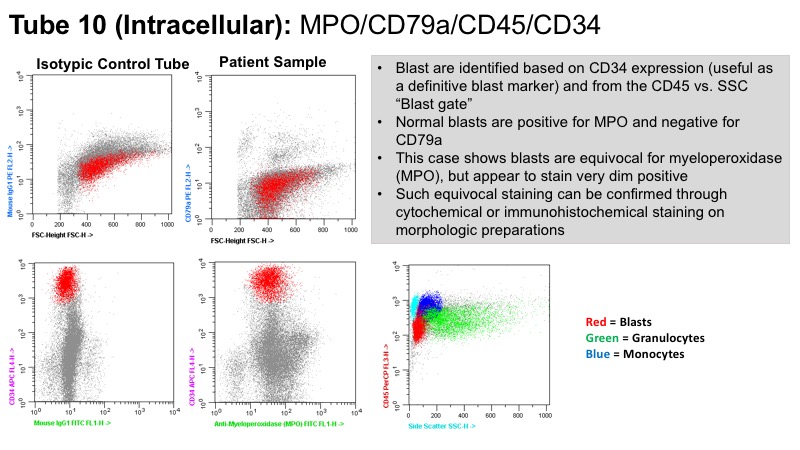
CORRECT: Is helpful in detecting immunophenotypic aberrancies in myeloblasts, such as expression of CD79a. There were no blast aberrancies present in this tube.
Continue
How is Blast Aberrancy Determined?
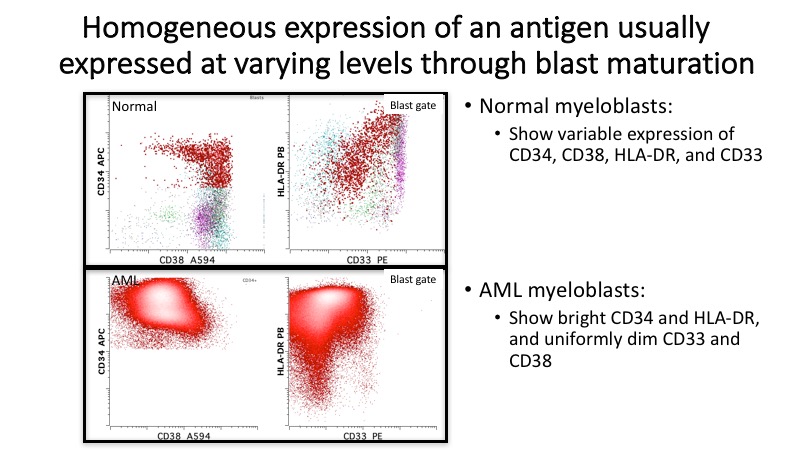
- Normal myeloblasts show a reproducible maturation pattern, with myeloid antigen expression at distinct levels depending on the stage of maturation.
- Aberrant myeloblasts (such as those found in AML) deviate from the normal immunophenotype.
- This case shows 15% myeloblasts with immunophenotypic aberrancies including an unusual expression pattern for CD15/CD33/CD34 as well as slightly dim expression of CD38 and HLA-DR.
- In addition to the aberrancy identified on the blasts, there is an expanded population of monocytes with increased variability of expression of CD11b, CD13, CD14, CD36, CD64 and HLA-DR, and with a minute proportion showing expression of CD34 and CD117.
- Please see following discussion for further information on normal and abnormal blast immunophenotypes.
Continue
Normal Myeloid Blast Maturational Patterns
- Once myeloid blasts have been specifically identified, one needs markers to distinguish normal from abnormal myeloid blasts.
- Abnormal blast immunophenotypes have been designated leukemia associated immunophenotypes (LAP or LAIP) in the literature.
- Identifying a LAP can be helpful in distinguishing marrsow regeneration from a myeloid stem cell disorder and is particularly important for MRD testing at follow-up post therapy.
- Detecting abnormalities on myeloid blasts requires recognition of normal patterns of antigen expression during myeloid maturation.
- Similar to the changes in morphology noted with maturation, hematopoietic cells demonstrate predictable, conserved changes in antigen expression with normal maturation.
- Such changes are seen at all stages of development with transition from early progenitor to early myeloid blasts to maturing myeloid, monocytic or erythroid elements.

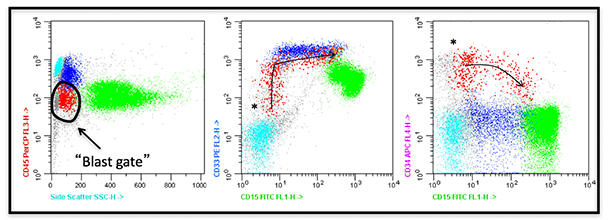
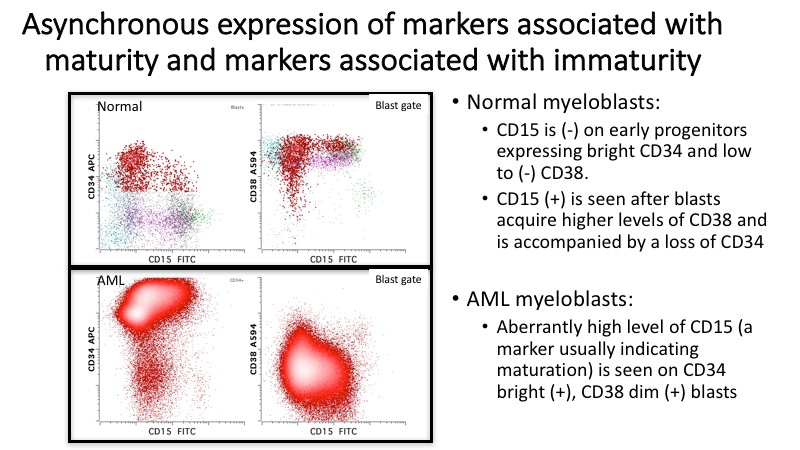
- Early progenitor cells (*) express very high levels of CD34 and low to absent CD38.
- With maturation, these early blasts gradually drop CD34 as they acquire CD38.
- As CD38 reaches maximal “blast” levels, CD34 drops precipitously and markers associated with maturation and differentiation (such as CD15 for myeloid differentiation and maturation), are acquired.
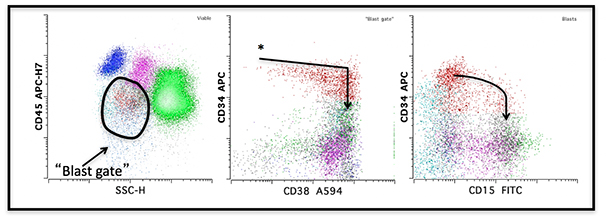
- Early progenitor cells (*) express very high levels of CD34, dim CD33 and no CD15.
- With maturation, these early blasts gradually drop CD34 as they acquire CD33 and CD15.
- Blasts are shown in red; granulocytes and monocytes are in green and blue, respectively.
- Small lymphocytes are shown in cyan.
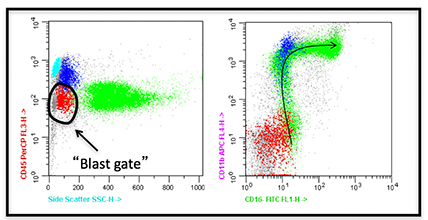
- Normal myeloblasts are negative for myeloid maturation markers, CD16 and CD11b.
- The arrow shows the normal granulocytic maturation curve.
- Blasts are shown in red; granulocytes and monocytes are in green and blue, respectively.
- Small lymphocytes are shown in cyan.
Continue
Abnormal Immunophenotype
- Abnormalities seen on myeloid progenitors in AML (and in other myeloid stem cell disorders) generally fall into one of 4 categories. Click on each to view:
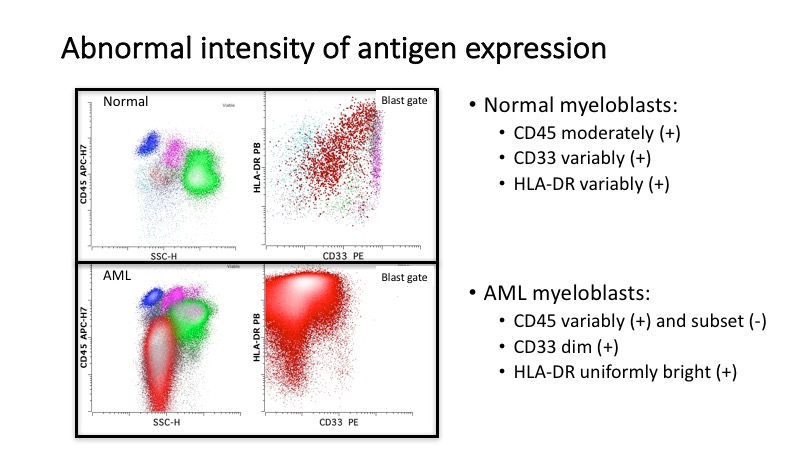
- • Abnormal intensity of antigen expression (increased, decreased or absent)
- • Asynchronous expression of markers associated with maturity and markers associated with immaturity
- • Homogeneous expression of an antigen usually expressed at varying levels through blast maturation
- • Expression of non-lineage antigens
- Identification of abnormal antigen expression is particularly helpful when performing evaluation for minimal residual disease (MRD) post therapy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Continue
Overall Immunophenotypic Findings in Case Example
- 15% population of variably-sized blasts with the following immunophenotype:
- CD34 (+), CD2 (few +), CD13 (+), CD15 (partial +), CD25 (few +), CD36 (few +), CD38 (variably +), CD45 (moderately +), CD64 (few +), CD117 (+), CD123 (variably +), HLA-DR (variably +), MPO (equivocal/dim +), TdT (-), other myeloid and lymphoid antigens pre-dominantly (-).
- 54% monocytes with variable expression of CD11b, CD13, CD14, CD36, and HLA-DR and with a minute proportion showing expression of CD34 and CD117
Question
INCORRECT:
Flow cytometry is not sufficient for establishing a diagnosis, as additional information derived from the bone marrow biopsy examination is required.
At this point the following interpretation could be rendered:
• An expanded population of immunophenotypically aberrant myeloblasts in a background of expanded monocytic cells with some aberrant features and some features of immaturity.
• Consistent with a high grade myeloid neoplasm with differential diagnoses including (but not limited to) evolving acute myeloid leukemia with monocytic differentiation or chronic myelomonocytic leukemia-2.
PARTIALLY CORRECT:
This answer is partially correct, since the peripheral blood blast percentage and morphology allow making a diagnosis of AML. However, additional information derived from cytogenetics is required to establish the final AML subtype, according to the WHO classification.
{kind=link}
CORRECT:
The information provided by bone marrow examination and cytogenetics offers the final, complete diagnosis of AML with inv(16).
{kind=link}
{kind=link}
{kind=link}
Continue
Final Diagnosis
Diagnosis
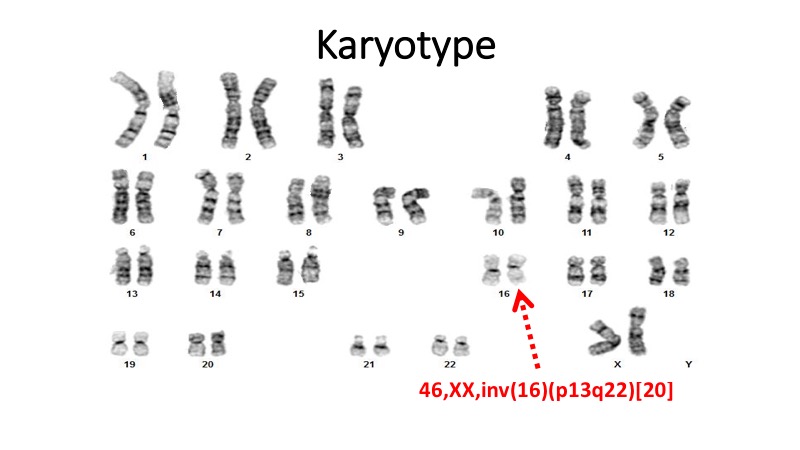
ACUTE MYELOID LEUKEMIA (AML) WITH INV(16)(p13q22)Definition
- A Core Binding Factor (CBF) Leukemia:
- Defined by a recurrent cytogenetic abnormality irrespective of blast count at diagnosis - inv(16)(p13q22) or t(16;16)(p13;q22).
- This is one of the genetic alterations that allow making a diagnosis of AML even with <20% blasts.
- WHO 2008 Classification Definition: Acute myelomonocytic leukemia with abnormal eosinophils (AML-M4Eo by FAB) in the bone marrow
Morphology
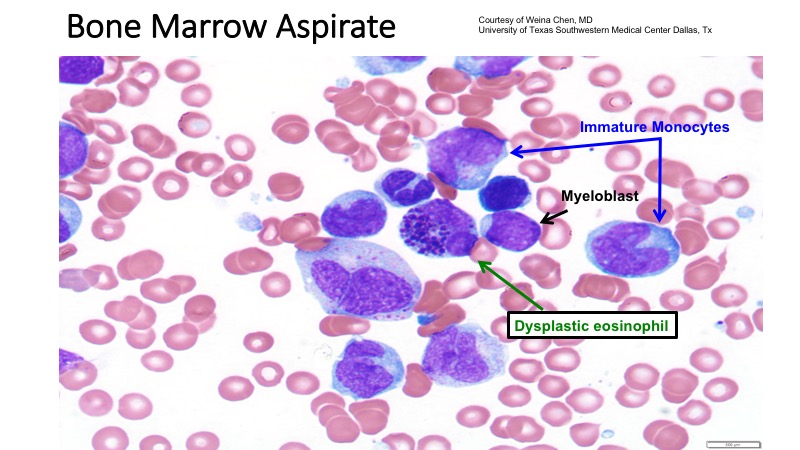
Peripheral Blood & Bone Marrow:- Heterogeneous neoplastic population of myeloblasts, monoblasts & promonocytes.
- Maturing granulocytes are sparse and do not show dysplasia.
- Hypercellular marrow often with more than 20% blasts
- May be lower than 20% in some cases
- Auer rods may be seen in blasts.
- Most striking abnormality: Eosinophils and eosinophilic promyelocytes and myelocytes have large immature basophilic granules.
Immunophenotype
- Double population of pathological cells:
- Myeloid blast cells: CD34, CD117, CD13, CD33, CD15, myeloperoxidase.
- Monocytic cells: CD4, CD11b, CD11c, CD14, CD64, CD36, lysozyme
- Aberrant coexpression of CD2 in the blast population and monocytic cells occurs in a subset of cases but it is not specific for this type of AML
Prognosis
- Overall good prognosis
- Good response to Cytarabine-based chemotherapy
- KIT mutations are present in approximately 30% of cases
- Worse overall survival and higher rates of relapse
- Trisomy 22 - Specific and seen in 10-15% cases favorable outcome
Continue
Learning Assessment
Now that you’ve completed the e-learning activity, assess your knowledge with the following graded questions.
Question 1
CORRECT:
Blast are typically identified based on CD34 expression and CD45/SSC “blast gate”. CD38, CD13, CD33, and HLA-DR are expressed in immunophenotypically normal myeloblasts, but may not serve as primary gating markers.
INCORRECT:
Please try again.
INCORRECT:
Please try again.
INCORRECT:
Please try again.
INCORRECT:
Please try again.
Question 2
INCORRECT:
Please try again.
INCORRECT:
Please try again.
INCORRECT:
Please try again.
CORRECT:
Flow cytometry is a critical part of evaluation for acute leukemia, as it confirms cells as blasts using specific markers; allows lineage assignment; allows determination of immunophenotypic aberrancies of blasts; detects the presence of very low levels of aberrant blasts in the absence of morphologic evidence of acute leukemia (minimal residual disease); and may assist in blast enumeration in the blood. However, several factors may confound blast enumeration by flow cytometry in the marrow, including hemodilution or partial lysis of erythroid precursors, which may artificially decrease or increase the blast percentage, respectively. As such, the most reliable method for blast enumeration in the marrow is morphology.
INCORRECT:
Please try again.
Continue
Summary
- Flow cytometry is a critical part of the diagnosis of AML
- Flow cytometry can facilitate:
- Blast identification
- Lineage assignment
- AML classification
- However, blast enumeration in the marrow should be done by morphology.
- Genetic information also assists with final classification, such as in the example of AML with inv16.
Suggested Reading
- Eds. Steven Swerdlow EC, Nancy Lee Harris, Elaine S. Jaffe, Stefano A. Pileri, Harald Stein, Jurgen Thiele, and James W. Vardiman. World Health Organization Classification of Tumors: WHO classification of tumors of haematopoietic and lymphoid tissues, 4th edition. Lyon, 2008.
- Wood BL. Myeloid malignancies: myelodysplastic syndromes, myeloproliferative disorders, and acute myeloid leukemia. Clin Lab Med. Sep 2007;27(3):551-575, vii.
- Craig FE, Foon KA. Flow cytometric immunophenotyping for hematologic neoplasms. Blood. Apr 15 2008;111(8):3941-3967.
- Al-Mawali A, Gillis D, Lewis I. The role of multiparameter flow cytometry for detection of minimal residual disease in acute myeloid leukemia. Am J Clin Pathol. Jan 2009;131(1):16-26.
- Wood BL, Arroz M, Barnett D, et al. 2006 Bethesda International Consensus recommendations on the immunophenotypic analysis of hematolymphoid neoplasia by flow cytometry: optimal reagents and reporting for the flow cytometric diagnosis of hematopoietic neoplasia. Cytometry B Clin Cytom. 2007;72 Suppl 1:S14-22.
- Kussick SJ, Wood BL. Using 4-color flow cytometry to identify abnormal myeloid populations. Arch Pathol Lab Med. Sep 2003;127(9):1140-1147.
End Case/Course