Multimer technology
In 1996, Altman et al. (1) demonstrated that the low affinity of a single peptide-MHC complex for its corresponding T cell receptor (TCR) was the primary reason initial attempts to stain T cells directly with their specific antigen had failed. TCRs have a low affinity for their peptide MHC counterparts, with an off-rate of only a few seconds (2). Monomeric MHC-TCR interactions were therefore too unstable to be exploited as an effective labeling technique. Tetramers of peptide plus MHC class I complexes, however, labeled CD8 T cells specifically by providing the required avidity to obtain a clear-cut cytometric signal. Combining multiple MHC molecules into one complex greatly increases binding stability so that today these MHC class I tetramers, generically known as multimers, have become widely used for the quantification of various antigen-specific CD8 T cell responses including those to tumor, bacterial, viral and auto antigens.
There are 3 different types of commercially available multimer reagents (Figure 1). The classic “tetramer” (Beckman Coulter, Miami FL) is composed of a soluble MHC class I or class II monomer with an antigen specific peptide of 8 to 10 amino acids non-covalently bound within the MHC grove in the presence of ß2-microglobulin. MHC-peptide monomeric complexes are biotinylated and converted to tetravalent structures by binding to (fluorochrome-conjugated) streptavidin, which has four biotin binding sites.
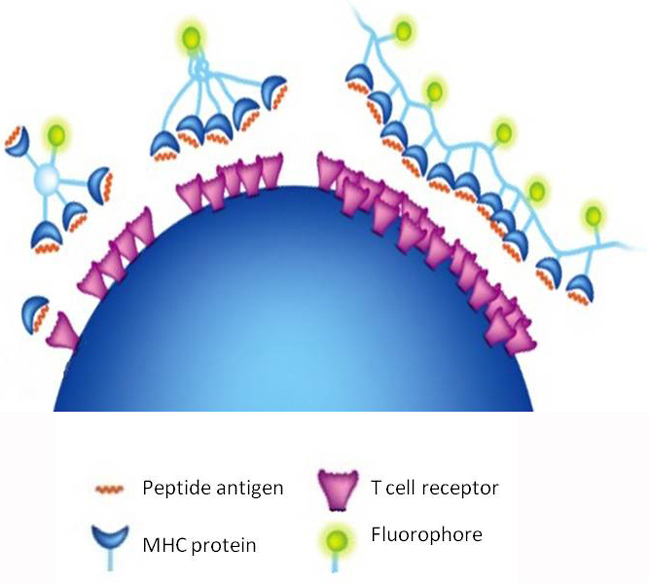
Figure 1.Three different types of commercially available multimer reagents. Far left, MHC class I molecule with peptide antigen non-covalently bound within the MHC grove complex and a T cell receptor. 2nd from left, the classic tetramer composed of four biotinylated MHC-peptide monomers converted to tetravalent structure by binding to fluorochrome-conjugated streptavidin. Center, the pentamer, a recombinant molecule composed of five MHC-peptide complexes in planar configuration which may have up to 5 fluorochromes attached. Right, dextramer, consisting of a dextran polymer backbone carrying typically greater than 10 MHC-peptide complexes and fluorochrome molecules. (Illustration courtesy of Liselotte Brix, Immudex)
Due to the rigid tetrahedral configuration of tetramer complexes, only three out of the four available MHC molecules are realistically available to bind simultaneously to the T cell surface. Improvements have focused on the development of strategies to increase the number of MHC molecules capable of binding to the cell and the number of fluorochromes attached to the complex. Pentamers (ProImmune, Oxford UK) comprise five MHC-peptide complexes assembled through a coiled-coil domain. Due to their planar configuration, all five MHC-peptide complexes face in the same direction resulting in a very high affinity for the complementary TCRs. Each pentamer also comprises up to five fluorescent or biotin tags for bright labeling. A third technology, dextramers (Immudex, Copenhagen, DK), consists of a dextran polymer backbone carrying MHC and fluorochrome molecules. Dextramers reagents carry more MHC molecules and more fluorochromes than any other conventional MHC multimers increasing their fluorescent intensity and improving their binding for low affinity TCR.
For flow cytometric enumeration of antigen specific CD8+ T cells, multimers typically in PE or APC are counterstained with CD8 after which lymphocytes are selected by gating on forward and side scatter. Class I restricted CD8 T cells are identified within the CD8(bright) subset. In practice, we prefer to include CD3 and a live dead viability dye (Figure 2) in the gating strategy. The forward and side scatter lymphocyte region is optimized using CD3 versus side scatter. This strategy excludes the CD8(dim) NK cells providing a more reliable enumeration of Class I restricted CD8 T cells. Since detection sensitivities of 0.01% are desirable, a viability dye is included to exclude dead cells, which can non-specifically bind multimers. A single platform tube containing beads, antibodies to CD3 and CD8 plus viability dye and optionally anti-CD4 is used to determine the absolute number of CD3+ CD8+ T cells. This count is multiplied by the percentage of antigen specific, multimers positive CD8 T cells to determine their absolute number. A harmonization study and consensus documents discussing these methods have been published (3, 4).
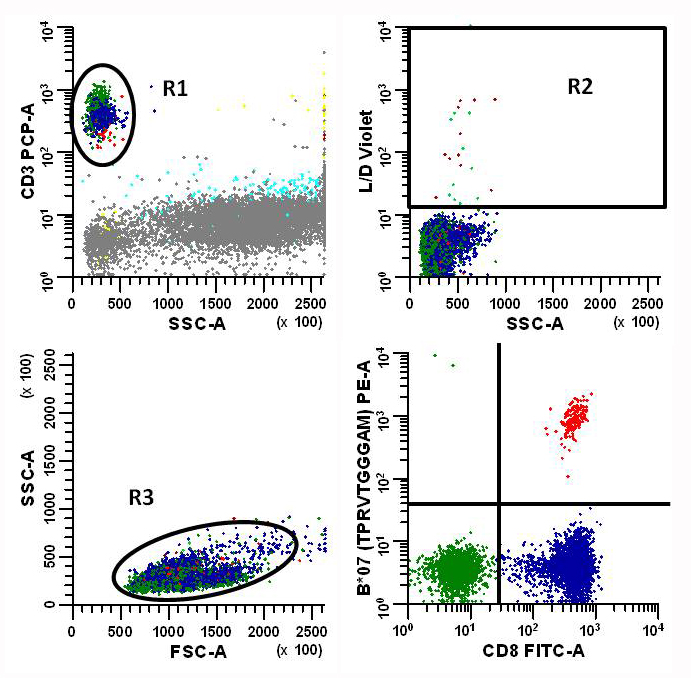
Figure 2. Flow cytometric analysis strategy for MHC Class I multimers. Data is initially gated on total CD3+ events, then passed through a viability gate (L/D violet) to exclude dead cells and finally cleaned up in a forward scatter (FSC) versus side scatter (SSC) histogram to remove aggregates and debris. The percentage of multimer+ (B*07 (TPRVTGGGAM)) CD8+ T cells is calculated and the absolute number is determined by multiplying this percentage by the absolute number of CD3+CD8+ T cells determined using a single platform tube. To increase sensitivity we try to obtain 25,000 CD3+CD8+ events per file.
At present, analysis of specific T cells with multimers is limited by the fact that only a selection of defined HLA alleles can be used, and that immuno-dominant peptides have to be predefined. While a variety of recombinant MHC class I molecules are now available, the selection is still somewhat limited. Thus both the HLA phenotype of the individual being tested and the immuno-dominant antigenic peptides for that MHC alleles must be know beforehand. For most of the HLA class I tetramer studies of vaccine efficacy, investigators have studied HLA-A2-restricted responses, since this HLA specificity is highly prevalent in many parts of the world. Identification of antigen specific CD4 cells has not been as successful, primarily due to there 10 to 100-fold lower frequency in the peripheral blood.
The multimer technology is beginning to enter the clinical laboratory for the detection of immune responses to CMV. As discussed below, patients receiving allogeneic hematopoietic stem cell transplants (allo HSCT) are at increased risk of developing CMV infection post transplant and enumerating the number of antigen specific CTL has been show to be useful in predicting recurrence of active disease which has significant morbidly and mortality in these immunocompromised patients.
CMV and immunosuppression
Human cytomegalovirus (CMV) is a herpes virus that infects 50 to 80% of individuals worldwide (5). After primary infection, which usually occurs in childhood, the virus remains latent in monocytes and hematopoietic stem cells and can replicate in endothelial cells. Transmission is through direct contact with body fluids, such as urine, saliva, or breast milk, it can also be spread through transplanted organs, blood transfusions and blood products. While infection is usually asymptomatic, it can be life-threatening for the immunocompromised patient, such as HIV-infected persons, the newborn, or for organ and bone marrow transplant recipients.
Infected persons develop lifelong humoral and cellular immunity to the virus, but reactivation is only prevented in healthy persons through immune surveillance by virus specific CD8+ cytotoxic and CD4+ T cells. When the cellular immune response is compromised, reactivation and clinical disease can occur. CMV interstitial pneumonia is the most common and severe infectious complication of HSCT patients. Onset is usually in the first 120 days. The principal finding on chest radiographs is an interstitial nodular infiltrate, associated with a rapid onset of fever, nonproductive cough and dyspnea (6).
Even with the introduction of potent antiviral agents, CMV infection continues to cause morbidity and mortality after transplantation. Prophylactic antiviral drugs such as ganciclovir reduce the incidence and severity of CMV infection and its complications after transplantation, but they are expensive and toxic. These antiviral agents produce bone marrow suppression associated with an increased risk of neutropenia and induction of drug resistance to the virus, along with bacterial and fungal infections. In order to reduce overexposure to ganciclovir, pre-emptive therapeutic strategies based on detection of CMV reactivation are used (5). Although pre-emptive ganciclovir offers a significant reduction in human CMV disease during the first 100 days after transplantation, there is an increasing recognition that late presentation of CMV disease can occur, which has a high mortality rate (7). The decision to administer antiviral therapy is currently based on the clinical risk and the detection of CMV by antigenemia assay or PCR. Monitoring to direct pre-emptive antiviral therapy can reduce the incidence of CMV disease and CMV-associated mortality, but the high sensitivity of these assays leads to treatment of many patients who would unlikely have progression to disease.
Monitoring CMV immune status to help direct antiviral treatment after HSCT may be of great value. In healthy individuals an equilibrium is established between CMV specific T cells and control of the persistent virus. When T cell function is impaired an equilibrium is not established and viral reactivation occurs. As discussed in the next section, recovery of CMV specific T-cell mediated immunity after HSCT is critical for protection against CMV disease. Therefore monitoring the number CMV specific CTL in blood may become another important variable to optimize antiviral therapy and minimize drug exposure.
Monitoring CMV specific T cells in HSCT Recipients
Several studies have examined CMV specific CD8+ T cells T cell recovery after allo HSCT using multimers and concluded that a failure to recover CMV specific CD8+ CTL HSCT is associated with the development of CMV disease. Cwynarski et al. (8) studied 24 recipients of allogeneic HSCT and found that recovery of CMV specific cytotoxic T cells to levels above 10 cells/µL was associated with protection from CMV disease. In patients given allografts from a sibling, when both the patient and donor were seropositive for CMV, recovery of CMV-specific CTL was rapid and reached up to 21% of all CD8+ T cells. Early reconstitution of CMV-specific immunity was not observed if either the donor or recipient was seronegative for CMV.
Gratama and colleagues have extensively used multimers to study recovery of CMV specific T cells responses post allogeneic HSCT. They initially reported on 27 HLA A*02+ patients (9). In this study, none of the CMV seronegative patients (n=9) developed a CMV specific CD8+ CTL response after HSCT. In contrast, the 13 of 14 CMV seropositive patients who developed detectable CTL by multimers never developed CMV disease. And most importantly, the 4 patients who developed CMV disease all failed to generate CMV specific CTL. The threshold associated with protection against disease in this study was 2 cells/µL. This and Cwynarski observations lead investigators to conclude that use of HLA-peptide multimers to quantify CMV CTL is valuable for studying T-cell responses after HSCT and is an easy and sensitive tool for identifying HSCT recipients at risk for developing CMV disease.
Following up on their earlier study Gratama et al. (10) undertook a multicenter prospective longitudinal clinical trial evaluating the use of multimers in monitoring CMV-specific CD8 CTL recovery after HSCT. Eighty-three CMV seropositive recipients patients were tested every 2 weeks from day 28 to day 100, and then every 2 to 4 weeks from day 101 to day 270. Unlike earlier trials which only used HLA A*02 multimers, A*01, A*02, B*07, B*08, B*35 HLA alleles were included. This increased coverage to 77% of whites, 48% of blacks and 42% of Asians. Delayed recovery of CMV specific T cells (defined as < 7 cells/µL in all blood samples during the first 65 days after transplantation) was found to be a significant risk factor for CMV-related complications compared to patients with rapid recoveries. These patients were 2.6 times more likely to develop recurrent or persistent CMV infection than patients showing rapid recovery. Other risk factors were examined for their association with recurrent or persistent CMV infection or disease; however, CMV-specific CTL counts were the only independent risk factor.
Value may not only come from monitoring CMV specific CTL recoveries in patients post transplant but also in the graft itself. Transplanters have long thought that antigen specific T cells in the HSCT could adoptively transfer protection at least initially while immunity develops in the recipient. In the Gratama 2001 study (9), they also looked at the number of CMV specific CTL in the graft and found an inverse correlation between the number of CTL transferred from the donor and the number of preemptive courses of ganciclovir. Conversely, T cell depletion and in particular, inclusion of anti-thymocyte globulin in the preparative regime for modified HSCT interfered with early recovery of CMV specific T cells and predisposed the patients for recurrent CMV infection and CMV disease.
Recently, the impact of CMV infection on acute myeloid leukemic recurrence was evaluated in patients undergoing HSCT (11). Surprisingly, the incidence of relapse at 10 years after transplant was significantly lower in patients with early CMV antigenemia. This study concluded that the detection of CMV antigenemia was a strong and independent predictor of reduced leukemic relapse translating into superior long-term survival in early and advanced stages of AML. While these authors did not evaluate T-cell immunity, a possible and intriguing mechanism by which CMV replication may be associated with a long-term anti-leukemic effect after HSCT is that the quality of the T-cell immune response to CMV may be a surrogate for the strength of donor T-cell mediated anti-leukemic effects. We are now looking at our multimers data to ascertain if a poor initial CMV immune response predicts relapse in patients with hematological malignancies.
In addition to enumerating antigen specific CTL, it may also be important to determine the functional capacity of the cells as measured by the percentage of multimer positive cells that are also capable of producing cytokines upon antigen stimulation. A downside of detecting antigen specific T cells by multimers is that this technique says nothing about the function of these cells. In fact, we have found in an influenza model that only half of the antigen specific T cells detected with by multimers were capable of proliferation or cytokine production (12). Detection of interferon gamma production by both CD4 and CD8 T cells using peptide pools derived from CMV proteins may in the future allow a finer dissection of the immune response to this virus without a need to know either the HLA type or the immuno-dominant peptides.
Conclusions
The development and commercialization of MHC class I multimers make the flow cytometric enumeration of antigen specific cytotoxic T lymphocytes simple and rapid. Currently the only limitations are that both the HLA type and the immuno-dominant peptides must be known. These reagents are finding their way into the monitoring of immune responses to infectious agents in patients receiving allo HSCT. As a consequence of the immunodeficiency and lack of immunosurveillance following transplant, latent viruses such as CMV may reactivate and cause disease. CMV disease following allo HSCT is a significant cause of morbidity and mortality and recovery of CMV specific CTL immunity after HSCT is critical for protection against disease. Depending on the study, recovery of between 2 and 10 CMV specific CTL per µL of blood early after transplantation has been found to be a significant predictor of those patients who will not develop CMV-related complications. While immunity develops anti-virals such as ganciclovir are used in preemptive antiviral strategies to control CMV replication. Although generally effective, these preemptive approaches are themselves immunosuppressive and often lead to overtreatment which is both costly and can result in the development of anti-viral resistant strains. The use of multimers to enumerate CMV specific CTL is likely to better optimize the administration of pre-emptive therapy, reducing costs and may in the long run be a predictor of disease relapse.

Paul K. Wallace.
Roswell Park Cancer Institute, Department of Flow and Image Cytometry, Elm & Carlton Streets, Buffalo, NY 14263
E-Mail: pkw@RPCIflow.org
References
1. Altman JD, Moss PA, Goulder PJ, Barouch DH, McHeyzer-Williams MG, Bell JI, et al. Phenotypic analysis of antigen-specific T lymphocytes. Science. 1996;274(5284):94-6.
2. Matsui K, Boniface JJ, Reay PA, Schild H, Fazekas de St Groth B, Davis MM. Low affinity interaction of peptide-MHC complexes with T cell receptors. Science. 1991;254(5039):1788-91.
3. Heijnen IA, Barnett D, Arroz MJ, Barry SM, Bonneville M, Brando B, et al. Enumeration of antigen-specific CD8+ T lymphocytes by single-platform, HLA tetramer-based flow cytometry: a European multicenter evaluation. Cytometry Part B, Clinical cytometry. 2004;62(1):1-13.
4. Britten CM, Janetzki S, Ben-Porat L, Clay TM, Kalos M, Maecker H, et al. Harmonization guidelines for HLA-peptide multimer assays derived from results of a large scale international proficiency panel of the Cancer Vaccine Consortium. Cancer immunology, immunotherapy. 2009;58(10):1701-13.
5. Boeckh M, Nichols WG, Papanicolaou G, Rubin R, Wingard JR, Zaia J. Cytomegalovirus in hematopoietic stem cell transplant recipients: Current status, known challenges, and future strategies. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation. 2003;9(9):543-58.
6. Ho M. Epidemiology of cytomegalovirus infections. Reviews of infectious diseases. 1990;12 Suppl 7:S701-10.
7. Boudreault AA, Xie H, Rakita RM, Scott JD, Davis CL, Boeckh M, et al. Risk factors for late-onset cytomegalovirus disease in donor seropositive/recipient seronegative kidney transplant recipients who receive antiviral prophylaxis. Transplant Infectious Disease. 2011;13(3):244-9.
8. Cwynarski K, Ainsworth J, Cobbold M, Wagner S, Mahendra P, Apperley J, et al. Direct visualization of cytomegalovirus-specific T-cell reconstitution after allogeneic stem cell transplantation. Blood. 2001;97(5):1232-40.
9. Gratama JW, van Esser JW, Lamers CH, Tournay C, Lowenberg B, Bolhuis RL, et al. Tetramer-based quantification of cytomegalovirus (CMV)-specific CD8+ T lymphocytes in T-cell-depleted stem cell grafts and after transplantation may identify patients at risk for progressive CMV infection. Blood. 2001;98(5):1358-64.
10. Gratama JW, Boeckh M, Nakamura R, Cornelissen JJ, Brooimans RA, Zaia JA, et al. Immune monitoring with iTAg MHC Tetramers for prediction of recurrent or persistent cytomegalovirus infection or disease in allogeneic hematopoietic stem cell transplant recipients: a prospective multicenter study. Blood. 2010;116(10):1655-62.
11. Elmaagacli AH, Steckel NK, Koldehoff M, Hegerfeldt Y, Trenschel R, Ditschkowski M, et al. Early human cytomegalovirus replication after transplantation is associated with a decreased relapse risk: evidence for a putative virus-versus-leukemia effect in acute myeloid leukemia patients. Blood. 2011;118(5):1402-12.
12. Bercovici N, Givan AL, Waugh MG, Fisher JL, Vernel-Pauillac F, Ernstoff MS, et al. Multiparameter precursor analysis of T-cell responses to antigen. Journal of immunological methods. 2003;276(1-2):5-17.
|