|
In recent years, flow cytometry has taken on much wider applications in areas of Haematology, which have traditionally utilised manual techniques. The measurement of feto-maternal haemorrhage by flow cytometry is one such area which is becoming more widely used in routine clinical practice. Although its use has been described since the late 1980’s, guidelines only became available in the UK in 1999, and testing has mainly been confined to reference centres. The cost effectiveness of implementing a flow cytometric approach, existence of staff with the relevant experience and knowledge to implement successfully, limited scientific evidence to support methodology or availability of reagents may have also contributed to a flow cytometric approach not being more widely used. In Jun 2010, the UK National external quality assessment scheme for FMH testing had 45 participants registered for Flow cytometry as compared to 200 participants registered for the ‘Kleihauer-Betke’ acid elution method.
Feto-maternal haemorrhage refers to the cross placental transfer of fetal red blood cells to the maternal circulation. This may occur during delivery, but therapeutic interventions, PV bleeding, falls or other trauma may also contribute. In rhesus negative mothers, this may cause sensitisation and maternal alloimmunisation of anti-D, resulting in haemolytic disease of the newborn in subsequent pregnancies. In order to prevent this, anti-D immunoglobulin is administered to rhesus negative women after such events and post delivery to prevent sensitisation. Routine antenatal anti-D prophylaxis (RAADP) is also offered. According to the National Institute of Clinical Excellence, using 2005 figures it was estimated that approximately 1% of women will still go on to develop anti-D despite being given anti-D immunoglobulin for sensitising events6. UK based community trials comparing Rhesus negative women not given RAADP (Control group) and those given RAADP (Treatment group) reported the sensitisation rate in the control group to be 0.95% compared to 0.35% in the treatment group6. This demonstrates a significant reduction in risk if RAADP is given. As a result, all Rhesus negative women in the UK are now offered prophylactic anti-D during the third trimester.
The volume of cross-placental bleeding which occurs is extremely unpredictable, although certain events are thought to be more likely to cause bleeding such as caesarean section, forceps delivery and manual removal of placenta1. A review of published cases between 1966 and 1997 by Giacoia reported that in 82% of cases of significant bleeds the causes were unknown3. A multi-centre study by Chen et al using 0.10% as a cut off for clinically significant FMH found 5.3 % of cases had a significant bleed and of those 52% had a caesarean section2. The variability of bleed volume and the inability to predict with any certainty the clinical scenarios more likely to cause significant FMH highlights the need to be able to accurately quantitate FMH, in order to calculate the dose of anti-D which is required to remove all rhesus D positive red cells from the maternal circulation, and prevent sensitisation.
The Flow cytometric methods employed measure the presence of fetal red cells in a maternal sample either using an antibody against fetal haemoglobin (HbF) or against the ‘D’ positive antigens on fetal red cells. Glycophorin A (CD235a) may also be included in the method to positively identify the red blood cell population.
The technique which uses a monoclonal antibody against HbF is slightly more technically demanding, due to cytoplasmic staining, and must include a means of being able to distinguish adult HbF from fetal HbF, but has the advantage of being able to quantitate fetal bleeds regardless of rhesus type of mother or baby. This may be a requirement in cases of still birth, intrauterine death or unexplained significant anaemia in the newborn. Such methods often utilise an antibody against Carbonic anhydrase. This is an enzyme which is present in adults RBC’s and only very late stage fetal cells, so is therefore useful in combination with anti-HbF to distinguish between maternal HbF and fetal HbF.
The approach using a monoclonal anti-D as a means of identifying FMH is a surface membrane technique, so is more straightforward and is not affected by an increased HbF level in the mother. However its use is limited to predicting the level of rhesus positive red cells in a rhesus negative sample. This may be useful in circumstances where the fetal group is not known and the HbF measurement remains positive even after anti-D prophylaxis. In such instances, if the anti-D method shows no evidence of a bleed then it is very probable that the fetus is rhesus negative.
The method described in this report utilises a direct staining approach with an anti-D FITC conjugated reagent to isolate Rhesus D positive fetal cells in the maternal sample.
The majority of samples tested in our laboratory are post delivery samples. It is recommended that a different sample is used to the one taken for blood grouping and screening. This is due to the theoretical risk that during centrifugation and blood grouping, the larger fetal red cells sitting closer to the plasma/RBC interface may be sampled preferentially, thereby underestimating the fetal bleed11. In our laboratory often only one sample is taken, therefore flow cytometry is performed prior to grouping the mother’s sample. In addition, a cord blood sample is taken at delivery and the ABO and rhesus type identified, so that only mothers of rhesus ‘D’ positive babies undergo flow cytometric testing. An alkali denaturation test (APT)8. is also performed on both maternal and cord samples. This differentiates between adult and fetal blood and confirms that mother and cord samples have been labelled correctly.
For Flow cytometry, samples are taken into EDTA and are thoroughly mixed before testing. For quantitative purposes the tests are performed in duplicate and an average of the two results used. For each patient two 50µl aliquots of whole blood are washed twice in fresh phosphate buffered saline pH 7.0 (PBS) using a ‘swing out’ centrifuge at 1000g for two minutes to minimise the number of white blood cells and platelets. The supernatant is removed at each stage with a pastette rather than decanting. After final washing the cells are resuspended in 1ml of PBS. With each batch of testing, controls are included, which are equivalent to 1.0%, 0.2% and 0.0% bleeds.
The antibody selected for identification of rhesus ‘D’ positive cells should ideally react with all D phenotypes which are capable of initiating an immune response, although many are unable to detect the DVI phenotype. However the rare DVI phenotype lacks the most immunogenic part of the rhesus D antigen4.
We use the BRAD3 anti-D FITC conjugated reagent produced by IBGRL, to identify ‘D’ positive red cells and for each patient we also include an isotype and fluorochrome matched negative control. (AEVZ negative control, IBGRL). A volume of 5µl is used for each reagent, to which 50µl of the red cell suspension is added. For an average red cell count, this volume and dilution equates to approximately 1 x 107 cells recommended by the antibody manufacturer. We have adapted the method slightly to include 2.5µl of CD45 (Leucocyte common antigen) to each tube. This enables any residual contaminating WBC’s to be removed from the red cell gate, thereby reducing the background caused by non-specific binding. After vortexing, the cells are incubated at 37oC in the dark for 30 minutes. They are then washed once in PBS and resuspended in 2mls PBS and analysed on the flow cytometer within one hour.
Flow cytometric analysis is performed on a BD FACS Canto II analyser using FACS Diva software. 250,000 events are acquired in each tube (500,000 events in total) and an average of the two tubes taken. Red blood cells are gated on the basis of their forward and side scatter characteristics on a log/log FSC/SSC dot plot. (Figure 1) Additional gating on a CD45/SSC dot plot is then applied and any contaminating leucocytes excluded using an invert (not) gate. The red cells are examined on a FITC labelled histogram, with the scale adjusted on the y axis to exaggerate the minor D positive peak. The 1% control sample is used to determine the position of the D positive red cells and a region set around this accordingly.
Figure 1:
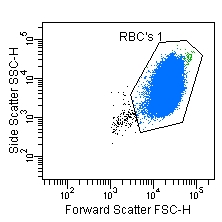
a): Forward and side scatter dot plot showing position of RBC population and gating position.
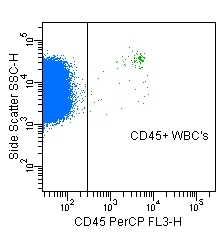
b): Dot plot showing separation of CD45+ WBC’s from CD45- RBC’s. Used to remove residual WBC’s from analysis and minimise background further.
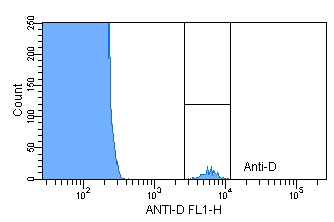
c): Histogram demonstrating 1% control and position of marker.
In order to calculate the volume of bleed, the background of the isotype matched control is subtracted from the number of events obtained in the ‘D’ positive region as recommended in the UK BCSH guidelines and the following calculation applied. This assumes that fetal cells are 22% larger than maternal cells and the maternal red cell volume is 1,800mls12.
Volume of fetal bleed (mls) = % fetal cells by flow cytometry x 18 x 1.22
The minimum standard dose of anti-D given at delivery in the UK is 500 international units (IU). This is sufficient to clear a bleed of up to 4mls from the maternal circulation. If the volume of FMH exceeds that covered by the standard dose, then supplementary doses should be given and follow up testing performed.
The method described has been employed within our laboratory since April 2007. Rather than using the acid elution method for screening, we use a more simplified flow cytometric technique whereby a single tube and only 100,000 events are analysed. This is followed up with a full quantitation if this screening test indicates a bleed greater than 2mls.
Since implementing a flow cytometric procedure, 3,587 screens have been performed in our laboratory over a 4 year period. Quantitations have been performed in 31 cases where the bleed exceeded 2ml. Of these, 22 cases (0.61%) had bleeds greater than 4 mls. This demonstrates a slighter lower significant bleed rate in our obstetric population as compared to the 1% quoted in the UK BCSH 2009 FMH guidelines.
During this period we have encountered three cases exhibiting an unusual phenomenon, whereby the histogram exhibits a broad peak situated in the negative region but shifted to the right. (Figure 2b) Repeats on initial and subsequent samples showed the same phenomenon. Examination of the patients’ blood grouping history identified one patient as having the partial D type: DAU-4. The second patient was a baby sample known to be a weak D, The third patient typed as rhesus negative. The sample was referred to the National blood service for specialist grouping techniques but no aberrant D type was detected. This illustrates that aberrant findings can occur with this method and there is a need for vigilance and that interpretation should occur in conjunction with the results obtained during blood grouping of antenatal patients.
Figure 2:
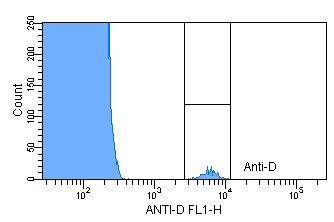
a) Position of Normal Rhesus D negative and positive peaks.
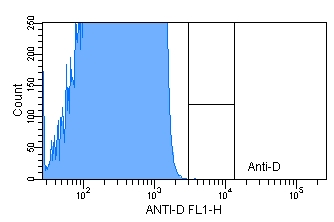
b) Plot depicting an aberrant peak shift.
This review is meant to provide a general overview of FMH testing and is not meant to be a guideline for flow cytometric analysis. For a more detailed knowledge, local and national guidelines related to estimation of Feto-maternal haemorrhage and anti-D prophylaxis should be referred to.

Ms. Rosalie Y Ward,
Chief Biomedical Scientist,
Flow Cytometry laboratory, Haematology department,
Sheffield Teaching Hospitals Foundation Trust, Sheffield, UK
References:
- Banerjee J, Banerjee S. J. (1989) Study of fetomaternal haemorrhage in relation to mode of delivery. Indian Med Assoc. 87(5):107-8.
- Chen J.C, Davis B.H, Wood B, Warzynski M.J. (2002) Multicenter clinical experience with flow cytometric method for fetomaternal haemorrhage detection. Cytometry (Clinical cytometry) 50, 285-290.
- Giacoia GP. (1997), Severe fetomaternal hemorrhage: a review. Obstet Gynecol Surv. 52(6):372-80.
- Lloyd-Evans. P, Guest. A.R, Voak. D, Scott. M.L, (1999) Detection of weak and DV1 red cells in D-negative mixtures by Flow Cytometry: Implications for feto-maternal haemorrhage quantitation and D typing policies for newborns. British Journal of Haematology, 104, 621-625.
- National blood service, Product insert for FITC conjugated Anti-D reagent for determination of Feto-maternal haemorrhage. (Product: BRAD3 anti-D FITC, Code:9433FI)
- National Institute for Health and Clinical Excellence, (Aug 2008), Routine antenatal anti-D prophylaxis for women who are rhesus D negative: (Review of NICE technology appraisal guidance 41.). www.nice.org.uk, NICE technology appraisal guideline 156.
- Sebring ES, Polesky HF. (1990) Fetomaternal hemorrhage: incidence, risk factors, time of occurrence, and clinical effects. Transfusion. 30(4):344-57.
- Thomas E, (2006) Simple Test for the Differential of Maternal and Fetal Bloods. Transfusion medicine 16 (Supplement 1), p42.
- UK National External Quality Assessment Scheme (FMH) Results return information.
- Uriel M, Subirá D, Plaza J, Castañón S, Cañamares M, Recasens JD. (2010) Identification of feto-maternal haemorrhage around labour using flow cytometry immunophenotyping.. Eur J Obstet Gynecol Reprod Biol. 151 (1), 20-5.
- Working party of the British Committee for standards in Haematology, Transfusion taskforce. Guidelines for the estimation of Fetomaternal haemorrhage. www.bcshguidelines.com.2009.
- Klein H. G, Anstee D.J. (Dec 2005) Mollison’s Blood transfusion in Clinical medicine. 11th Edition edition. Wiley-Blackwell publishers.
|