Laboratory and Clinical Practice for Monitoring Sepsis with Neutrophil CD64 Index: Seven Year Experience at Cincinnati Children’s Hospital Medical Center (CCHMC)
Diagnosis and management of bacterial infections are heavily dependent upon the availability of accurate lab tests in concert with clinical history and symptoms. Generally, the most common laboratory tests performed to evaluate patients with suspected sepsis are: white blood cell count and differential, C- reactive protein, erythrocyte sedimentation rate, blood cultures and procalcitonin. Prior to 2005, CCHMC physicians in the Division of Neonatology relied primarily on clinical judgment, white blood cell counts and differential, and blood cultures to evaluate potentially infected infants. An evaluation of our own internal data demonstrated that this approach was failing to identify a significant portion of infected infants and promoted the use of excessive antibiotics in uninfected infants. Therefore, we set out to identify an improved method for evaluating potentially infected infants that would have a high sensitivity and negative predictive value, fast turnaround time, minimal blood volume, and minimal cost. After a thorough evaluation of the literature, it was decided that neutrophil CD64 was the best possible candidate to meet all of our requirements. The process to bring a new home brew assay into the clinical laboratory is initially expensive and involves lengthy developmental steps over a period of months and even years to ensure testing validity. There are also concerns that home brew assays are difficult to standardize between laboratories that may be testing the same biomarker. Consequently, most clinical laboratories hesitate to purse this venture especially when a company has already invested expense, time and steps necessary to bring a clinical assay to market. For that reason, the Division of Neonatology partnered with the CCHMC Flow Cytometry laboratory in evaluating the Leuko64TM kit procedure, developed by Trillium Diagnostics, LLC, and implementing it in clinical practice.1-4
The neutrophil CD64 assay quantitates the level of neutrophil CD64 expression. Increased neutrophil CD64 levels are found in response to inflammation and tissue injury as a consequence of mediators such as interferon-gamma and G-CSF.5 Model attributes that one considers in an ideal clinical test ought to exhibit minimal specimen volume, simplicity of procedure, stability of biomarker measured, quantitatively assessed, availability of negative and positive controls, rapid turn-around time, results similar between laboratories, and from an administrative perspective, low direct cost.
The neutrophil CD64 assay can be performed and reported easily within 60 minutes. Briefly, an antibody cocktail, containing fluorescently labeled CD163 and 2 clones of CD64, is mixed with 50mcL peripheral blood (PB, white blood cell count <25,000/mcL) for 10 min followed by 15 minute incubation with an RBC lyse reagent and then the addition of a bead suspension, for instrument calibration and interassay standardization, prior to analysis on a flow cytometer. Our laboratory first used a FACSCaliburTM before it was replaced recently with a FACSCantoTM II flow cytometer (BD Biosciences, San Jose, CA).
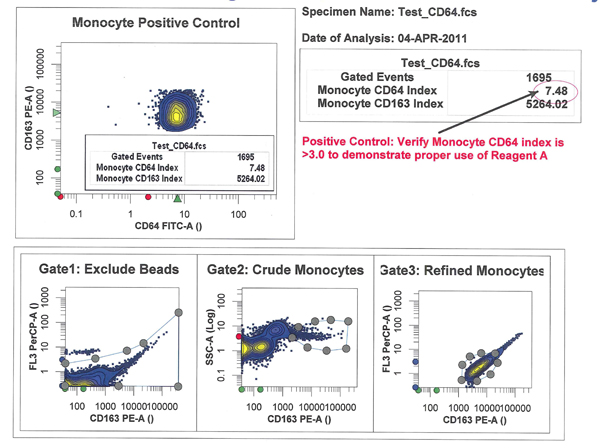
Data analysis is performed to define the neutrophil population using software that determines the neutrophil CD64 index by the ratio of linearized median fluorescence intensity of neutrophils to a FITC bead suspension signal (Figure 1). Each PB sample provides an internal negative control (lymphocytes) and internal positive control (monocytes). Lymphocytes must have a CD64 index of <1 and monocytes an index of >3 for the internal controls to be considered valid (Figures 2-3). The importance of quality laboratory work cannot be over emphasized and for that reason, in our hands, an additional normal PB control sample is tested daily for QC purposes to ensure accuracy and precision of test results.
Figure 1
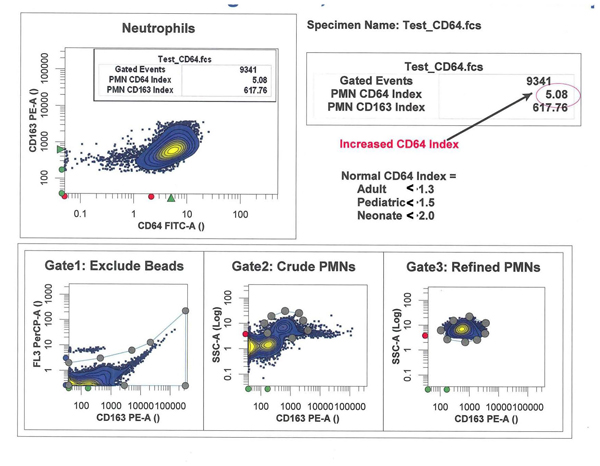
Figure 2
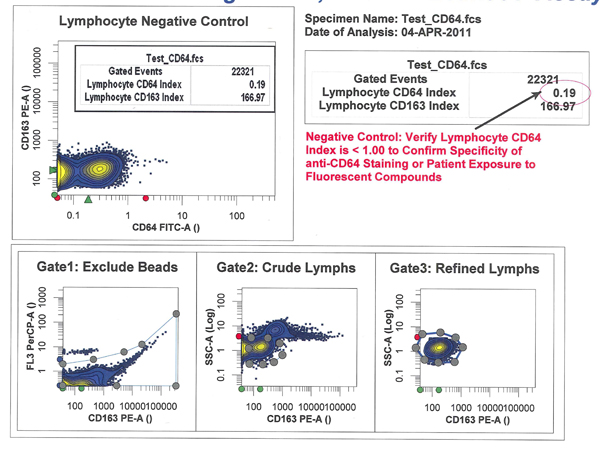
Figure 3
Essential to good laboratory practice, validation of any new test methodology is required under Clinical Laboratory Improvement Amendments (CLIA) to establish evidence that provides a high degree of assurance that a product, such as the CD64 assay, accomplishes its intended requirements and conditions.6-7 Performance characteristics reported by companies must be viewed as general guidelines showing how an assay should perform under optimum circumstances. For this reason, we elected to take this avenue to assess for ourselves the manufacturer’s claims of the CD64 assay are confirmed, accurate and dependable. Assay validation is not just a CLIA requirement, but is an integral part of good patient care.
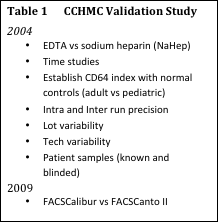 |
Our validation involved several steps to determine the assay’s legitimacy (Table 1). EDTA and sodium heparin PB specimens were tested at various times after collection. Results demonstrated that both anticoagulants were acceptable and the neutrophil CD64 marker was stable up to 48 hours (Table 2). PB from healthy adults was collected to define the normal neutrophil CD64 index. Similarly, this exercise was repeated using a different kit lot number confirming adult CD64 index and substantiating minimal lot-to-lot variation (Table 3). Intra and inter-assay runs established acceptable coefficient of variation (CV). Eight technologists were assigned to perform the CD64 test and analysis from a single specimen to demonstrate variability between staff. Another exercise performed was to have three of our staff independently analyze a single listmode file to determine problems or discrepancies. Here again, results were encouraging with an acceptable CV. This proves the assay’s bead suspension used for instrument calibration and interassay fluorescence standardization coupled with automated software, certainly removes data analysis subjectivity between multiple technical staff.
Before we offered CD64 assay clinically, an essential part of our validation study was to gather CD64 data from healthy children and neonates and from patients known to have infection defined by either positive cultures or clinical illness requiring >5 days of antibiotics. This analysis produced an abnormal CD64 index in our laboratory of >1.5 in pediatric patients and >2.0 in neonates.
Since 2005 and after appropriate validation, the CD64 assay has been used in over 1,500 infection evaluations in infants and the use of CD64 has increased each year. For quality control purposes, we have monitored the efficacy of the CD64 assay in identifying infected and non-infected patients. Consistent with previously published studies, the sensitivity and negative predictive value of the neutrophil CD64 assay has been consistently greater than 90% in identifying infected and non-infected infants. In fact, our analysis has found only 3 infants with culture positive infection that had a normal CD64 index. Two of these infants had blood cultures that were positive for Staphylococcus epidermidis and one had a positive blood culture that was obtained from a colonized central line.
Most CD64 analyses are completed with results reported back to the health care team within 3-4 hours. CD64 measurements can be completed with less than 0.5 ml of blood which makes this assay particularly appealing for evaluation of premature infants. In addition, the high specificity of the CD64 assay has made it particularly useful in the evaluation of complex and critically ill patients where it is difficult to determine if their clinical symptoms are due to an infection or their primary diagnosis.
In summary, the neutrophil CD64 assay, using the Leuko64TM kit, was thoroughly validated at CCHMC and proved to be a reliable assay. In clinical use, CD64 has significantly improved our evaluation of potentially infected infants and its use is currently being expanded to the pediatric population. However, full potential of the neutrophil CD64 assay is limited by the current time constraints of flow cytometry laboratory services and ultimately this assay will need to be transitioned to the main clinical laboratory before it can be implemented as part of every infection evaluation in the hospital.
|
|
|
Daniel Marmer, M.S., MT(ASCP)
Manager, Clinical Flow Cytometry Core Facility
Cincinnati Children's Hospital Medical Center
Cancer and Blood Diseases Institute Laboratory
Cincinnati, OH
|
Paul S. Kingma, MD, PhD
Section of Neonatology, Perinatal and Pulmonary Biology,
Cincinnati Children's Hospital Medical Center
Cincinnati, OH
|
References:
1. Davis BH. Improved diagnostic approaches to infection/sepsis detection. Expert Rev Mol Diagn. 2005;5:193-207.
2. Davis BH, Bigelow NC. Comparison or neutrophil CD64 expression, manual myeloid immaturity counts, and automated hematology analyzer flags as indicators of infection or sepsis. La Hematol. 2005; 11(2):137-147.
3. Davis, BH, Olsen SH, Ahmad E, Bigelow NC. Neutrophil CD64 is an improved indicator of infection or sepsis in emergency department patients. Arch Pathol Lab Med 2006;130:654-661.
4. Ng PC. Diagnostic markers of infection in neonates. Arch Dis Child Fetal Neonatal Ed. 2004;89:F229-F235.
5. Package insert. Leuko64TM Assay for detection of inflammation and tissue injury. 2009, LK64-v7. Trillium Diagnostics, LLC, Brewer, Maine.
6. National Committee on Clinical Laboratory Standards. Method Comparison and Bias Estimation Using Patient Samples; Approved Guideline-Second Edition. Wayne, PA: National Committee on Clinical Laboratory Standards; 2002. NCCLS document EP9-A2.
7. National Committee on Clinical Laboratory Standards. Preliminary Evaluation of Quantitative Clinical Laboratory Methods; Approved Guidelines-Second Edition. Wayne, PA: National Committee on Clinical Laboratory Standards; 2002. NCCLS document EP10-A2.