Ask an Expert
Back to Categories
What are the essential components in a clinical flow cytometry report for leukemia and lymphoma immunophenotyping?
There are many areas where the laboratory can communicate important information to the clinician in a report issued from flow cytometry in the analysis and interpretation of flow cytometry results. Several documents have been prepared to address these issues. The U.S. Canadian consensus guidelines first published in 19971 and updated at the Bethesda conference in 20062 are the most comprehensive and form the basis of this response. Additionally, CAP requirements have been noted3 and recommendations by the French GTLLF and GEIL on standardization of dot plot colors are discussed4 which will have importance for those laboratories that include such plots in their reports.
The recommendations as reported by the Bethesda consensus conference2 are shown in Table 1 and are separated into either required or optional and cover patient demographics, sample information and preparation, data analysis and interpretation and finally laboratory information and elements specific for U.S. laboratories.
For reporting, the key points that should be covered in the report are appropriate documentation allowing tracking of the sample date and time and other relevant samples taken at the same time (e.g. cytogenetics, core biopsy). The data is usually readily available in the hospital or laboratory information system and does not need to be typed directly into the report. Sample type (blood, marrow, lymph node etc.) and viability are key components of the report, particularly in aged or tissue samples. However, this may not be necessary for fresh blood and bone marrow. All antibodies tested should be reported in addition to the percentage of abnormal cells relative to a defined population (e.g. 30% lymphocytes, of white blood cells, or of all nucleated cells). However, the reporting of numerical data for each antigen is neither necessary nor recommended, as this tends to produce a large report that is often difficult to interpret. More importantly, a qualitative description of the abnormal population, if present, transmits clearer information to the requesting clinician. This information should include the fluorescence distribution of the cells of interest (negative/positive/partial) and also fluorescence intensity for relevant markers. This requirement, which is also used by CAP in their FL3 leukemia and lymphoma quality assurance survey, has caused significant confusion for many laboratories. A sample report is included at the end of this discussion and in Figure 1.
In the interpretation of the flow data, it is imperative to record any limitations. For example, on receipt of a bone marrow sample, note if it is clotted or a blood sample is hemolyzed. For tissue samples, in a lymph node with poor viability, a cytospin may show a population of large cells that are non-viable leaving behind only residual normal lymphocytes. A comment that the flow cytometry result may not be representative should be included.
In samples where no abnormal population is found, a description of the cell types within the sample should be reported along with any observations that may affect the sample result, for example, absence of nucleated red blood cells in a bone marrow sample coupled with strong CD15/CD16 expression on granulocytes would suggest peripheral blood contamination and would help to explain differences in percentages of abnormal cells reported by flow cytometry versus a bone marrow aspirate or biopsy result.
When an abnormal phenotype is detected, an interpretive comment should be given. However, it should be restricted to within the limits of the information available. For example, if a fine needle biopsy of a lymph node with limited cells shows a CD5(-)/CD10(-) light chain-restricted B-cell population, noting the presence of a lymphoproliferative disorder without further subclassification may be all that the laboratory can provide. However, a sample showing a sCD3(-)/cCD3(+)/CD34(+) population that is negative for CD4, CD8, and CD1a, but expressing myeloid-associated markers, a very specific comment noting that this phenotype is associated with an early progenitor T-cell leukemia/lymphoma provides crucial information to the attending clinician. Increasingly, surface phenotypes that show a strong association with recurrent cytogenetic translocations are becoming evident. For example, expression of CD19 on myeloblasts is associated with t(8;21) AML5, and absent or reduced expression of CD9 and CD20 in childhood B-ALL is associated with t(12;21)6. If the laboratory is performing rare event analysis, e.g., minimal residual disease (MRD) or paroxysmal nocturnal hemoglobinuria (PNH) testing, it is essential to report the lower level of quantitation that has been verified by the laboratory.
For those laboratories that include dot plots with their report, consideration should be given to using standardized colors, as recommended by the French GTLLF and GEIL groups7, and indorsed by the more recent ICSH/ICCS Workgroup5. These recommendations define subpopulations of CD45 versus SSC with lymphocytes (magenta) monocytes (green) granulocytes (red) and "blast region" (cyan).
For laboratories within the United States, it is also necessary to document Current Procedural Terminology (CPT) codes for billing and include an FDA statement related to laboratory developed tests which are not FDA approved. This is also a CAP requirement and may have different language3. Other jurisdictions may have similar or other legal requirements.
Included in U.S. "This test was developed and its performance characteristics determined by (laboratory name). It has not been cleared or approved by the US Food and Drug Administration."

Additional CAP comment
"FDA does not require this test to go through premarket FDA review. This test is used for clinical purposes. It should not be regarded as investigational or for research. This laboratory is certified under the Clinical Laboratory Improvement Amendments (CLIA) as qualified to perform high complexity clinical laboratory testing."
References:
1:Braylan RC, Atwater SK, Diamond L, Hassett JM, Johnson M, Kidd PJ,Leith C, Nguyen D. U.S.-Canadian consensus recommendations on
the immunophenotypic analysis of hematologic neoplasia by flow cytometry: Data reporting. Cytometry 1997;30:245-248.
2: Wood BL, Arroz M, Barnett D, DiGiuseppe J, Greig B, Kussick SJ, Oldaker T, Shenkin M, Stone E, Wallace P. 2006 Bethesda International Consensus recommendations on the immunophenotypic analysis of hematolymphoid neoplasia by flow cytometry: optimal reagents and reporting for the flow cytometric diagnosis of hematopoietic neoplasia. Cytometry B Clin Cytom. 2007;72 Suppl 1:S14-22.
3: CAP flow cytometry checklist, 07.28.2015. www.cap.org
4: Arnoulet C, Bene MC, Durrieu F, Feuillard J, Fossat C, Husson B, Jouault H, Maynadie M, Lacombe F. Four- and five-color flow cytometry analysis of leukocyte differentiation pathways in normal bone marrow: a reference document based on a systematic approach by the GTLLF and GEIL. Cytometry B Clin Cytom. 2010 Jan;78(1):4-10. doi: 10.1002/cyto.b.20484.
5: Kita K, Nakase K, Miwa H, Masuya M, Nishii K, Morita N, Takakura N, Otsuji A, Shirakawa S, Ueda T, et al. Phenotypical characteristics of acute myelocytic leukemia associated with the t(8;21)(q22;q22) chromosomal abnormality: frequent expression of immature B-cell antigen CD19 together with stem cell antigen CD34. Blood. 1992 Jul 15;80(2):470-7.
6: Borowitz MJ, Rubnitz J, Nash M, Pullen DJ, Camitta B. Surface antigen phenotype can predict TEL-AML1 rearrangement in childhood B-precursor ALL: a Pediatric Oncology Group study. Leukemia. 1998 Nov;12(11):1764-70.
7: ICSH/ICCS Workgroup. Validation of cell-based fluorescence assays: practice guidelines from the International Council for Standardization of Haematology and International Clinical Cytometry Society. Cytometry B Clin Cytom. 2013 Sep-Oct;84(5):281.
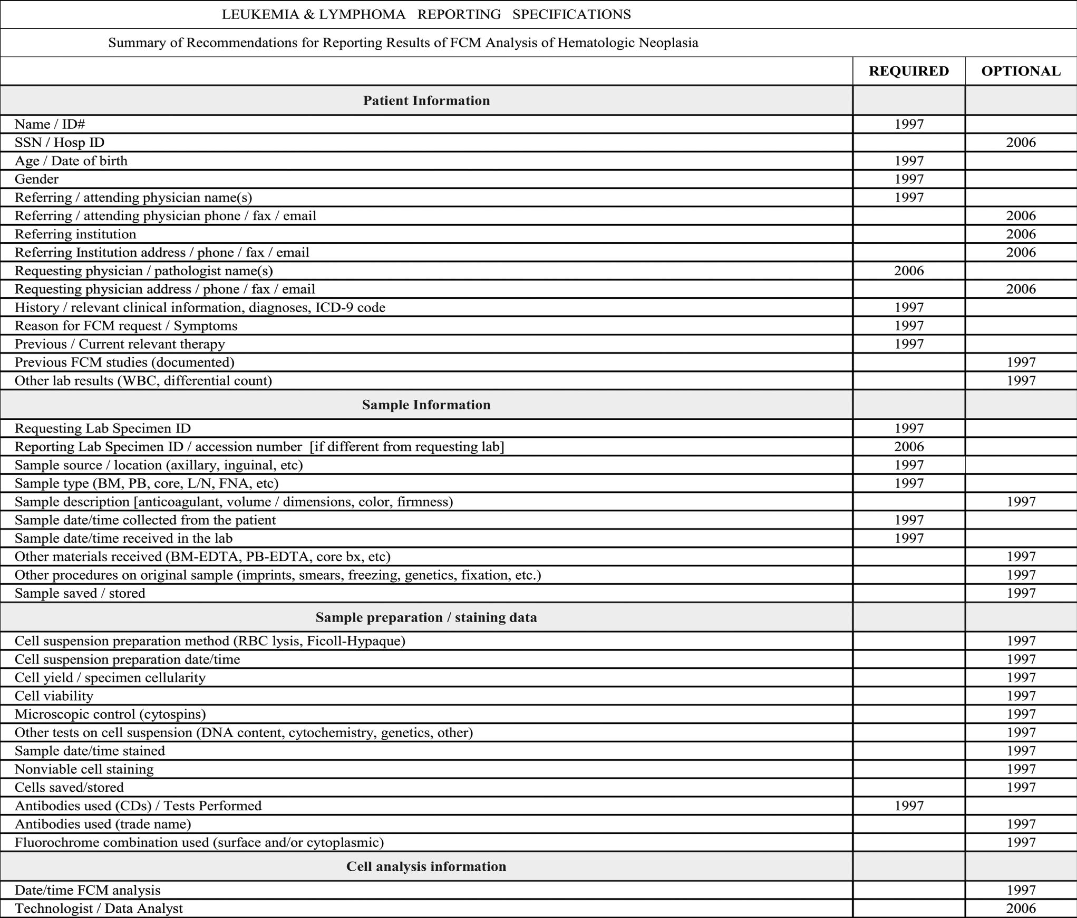

Each element of the report is indicated as being 'required' or 'optional'. Recommendations from the 1997 consensus conference (Cytometry (1997) 30: 245-248) are indicated by the designation '1997', and those from the 2006 consensus conference by the designation '2006'.
Author: Mike Keeney