Ask an Expert
Back to Categories
How can flow cytometry be used to test for autoimmune lymphoproliferative syndrome (ALPS)?
Autoimmune lymphoproliferative syndrome (ALPS) is characterized by defective lymphocytic homeostasis leading to dysregulation of the immune system. In ALPS, lymphocytes have aberrant survival causing non-malignant lymphoid proliferation. Although rare, patients also have increased risk of malignancy. ALPS is caused by defects in genes of the FAS pathway of apoptosis (FAS, FASLG, CASP10). ALPS usually presents in early childhood (median age 3 years). The typical patient is a usually otherwise healthy child who develops persistent lymphadenopathy and/or hepatosplenomegaly along with immune cytopenias. Recurrent infections are not commonly seen. Most often, the lymphoproliferation will improve over time (after 20 years of age, 66% of patients will have significant improvement).
The revised diagnostic criteria for ALPS (2009) are as follows:
Required criteria:
1. Chronic (>6 months), nonmalignant, noninfectious lymphadenopathy and/or splenomegaly.
2. Elevated CD3+/TCR??+/CD4-/CD8- cells (>1.5% of total lymphocytes or > 2.5% of CD3+ lymphocytes) in a setting of normal or elevated lymphocyte counts.
Primary accessory criteria:
1. Defective lymphocyte apoptosis in 2 separate assays.
2. Somatic or germline pathogenic mutation in FAS, FASLG or CASP10.
Secondary accessory criteria:
1. Elevated plasma soluble FASL levels (>200pg/mL), plasma IL-10 levels (>20pg/mL), serum or plasma vitamin B12 levels (>1500 ng/L), or plasma IL-18 levels (>500pg/mL).
2. Autoimmune cytopenias with elevated IgG levels (polyclonal hypergammaglobulinemia).
3. Family history of nonmalignant /noninfectious lymphoproliferations with or without autoimmunity.
4. Typical immunohistologic findings as reviewed by a hematopathologist.
Definitive diagnosis requires both required criteria plus one primary accessory criterion. A probable diagnosis is made if both required criteria, plus one secondary accessory criterion are present.
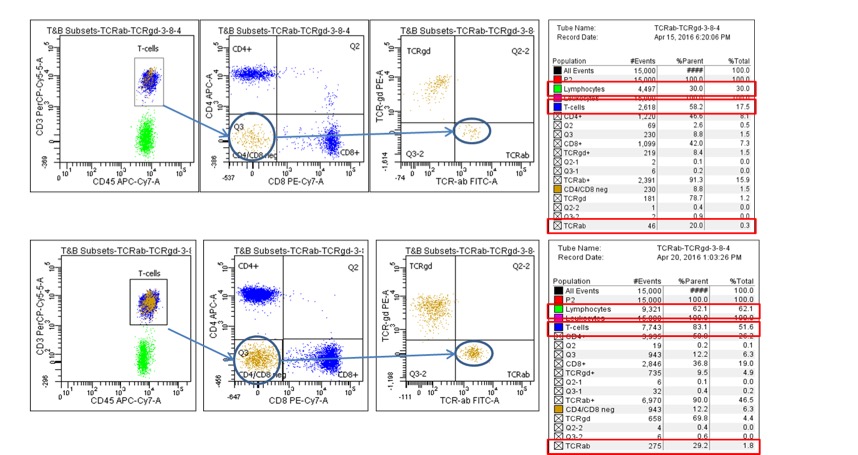
p>Flow cytometry plays a crucial role in enumerating the abnormal cells in required criterion #2 above. One approach is to use a tube that includes antibodies to CD45, CD3, CD4, CD8, TCRαβ, and TCRγδ (see Figure 1 below). First lymphocytes are gated using CD45/side scatter. Then by sequential gating, T cells are identified by CD3, and the CD4-/CD8- [double negative (DNT)] subset of T cells are gated. Then, the percentage of TCRαβ+ DNT cells is calculated. It is critical to distinguish these cells from normal TCRγδ(+) cells that are also negative for CD4 and CD8, such that they are not included in the calculation. In Figure 1, the top panel shows normal levels of DNT alpha;β cells (1.7% of T-cells and 1.0% of lymphocytes). The bottom panel shows increased levels of DNT alpha;β cells (3.6% of T-cells and 3.0% of lymphocytes).Figure 1:
Further Reading:
1. Oliveira JS (2013) The expanding spectrum of the autoimmune lymphoproliferative syndromes. Curr Opin Pediatr. 25:722-729.
2. Bleesing JJH, Johnson J, Zhang K (2014) Autoimmune lymphoproliferative syndrome. GeneReviews. Sep 2014.
3. Li P, Huang P, Yang Y, et al. (2016) Updated understanding of autoimmune lymphoproliferative syndrome (ALPS). Clin Rev Allergy Immunol. 50:55-63.
Author: Joy Punia