Ask an Expert
Back to Categories
How can mature and immature monocytes be distinguished by flow cytometry?
Monocytic cells have characteristic immunophenotypic features. Changes in immunophenotype parallel the changes seen in antigen expression as monocytic cells transition from immature monocytic precursors (monoblasts and promonocytes) to mature monocytic cells. In addition, changes in antigenic expression may be seen on mature monocytic cells with activation. A comprehensive understanding of immunophenotypic patterns associated with monocytic maturation and activation can assist with identification and separation of different monocytic subsets.
Monocytic maturation:
Monocytic cells at all stages of maturation express high levels of CD4, CD33, and CD64. Although these markers may be seen at intermediate levels on immature myeloid cells (promyelocytes), the level of expression of these markers on monocytic cells is typically higher (see Figure 1). The most immature monocytic cells (monoblasts and promonocyte) will express bright HLA-DR but will be low to negative for CD13 and CD14 expression. As monocytic cells mature they acquire increasing levels of CD13 and CD14 with high levels of CD13 and CD14 expressed by mature monocytic cells. The level of HLA-DR on mature monocytic cells can vary with activation state and variable CD15 expression is seen on monocytic cells at different stages of maturation.
With regard to CD14, it is important to note that the CD14 staining pattern is clone dependent. CD14 is typically negative on monoblasts; however, some anti-CD14 clones recognize mature monocytic cells only while others recognize promonocytes and mature monocytes (Yang et al 2005). Understanding the performance characteristics of the anti-CD14 clone you use in your laboratory is critical.
Monocytic populations in myeloid stem cell neoplasms with monocytosis:
As with all neoplastic cells, neoplastic monocytic cells do not always follow the rules (Xu et al. 2005). Neoplastic monocytic cells present in myeloid stem cell neoplasms (MSN) with monocytosis such as chronic myelomonocytic leukemia (CMML) and acute myeloid leukemia with monocytic differentiation (AML-Mo) may show a relative increase in monocytic cells and aberrant (increased or decreased intensity) expression of markers typically expressed by monocytic cells. CD56 may be aberrantly expressed on monocytic populations in MSN with monocytosis but expression of this marker is not specific and may be seen in reactive settings.
In cases with increased numbers of monocytic blast equivalents by morphology, monocyte populations with decreased or absent CD14 expression may be seen by flow cytometry. However, it is important be aware that although absence of CD14 on a monocytic population by flow cytometry typically correlates with a less mature state, abnormal monoblasts or promonocytes may not always be CD14 negative. Correlation with morphology is always required to define and accurately enumerate monocytic blast equivalents.
Identifying populations of immature monocytic cells by flow cytometry can be particularly challenging in cases with underlying myeloid dysplasia as dysplastic myeloid precursors show aberrant expression of myelomonocytic antigens and may be a challenge to reliably separate from immature monocytic cells by flow cytometry. Care should be taken to avoid erroneously classifying dysplastic myeloid precursors as immature monocytic blast equivalents in such cases and morphology can be a useful tool in this regard.
Finally, it should be noted that in MSN with monocytosis, the monocytic cells in the peripheral blood may be more mature than the monocytic component present in the marrow (see Figure 2). In MSN with monocytosis and less than 20% blast equivalents in the peripheral blood, evaluation of the marrow is critical for accurate diagnosis.
Classical versus non-classical monocytes:
Circulating monocytic cells predominantly consist of classical monocytic cells that express high levels of CD14 without CD16. Classical monocytic cells typically comprise 80-85% of the monocytic cells in the peripheral blood of healthy control subjects. The remaining monocytic cells consist of intermediate and non-classical monocytic cells. Intermediate monocytic cells show increased expression of CD16 while non-classical monocytic cells show expression of CD16 with decreased expression of CD14 (Mukerjee et al 2015). Although non-classical monocytes can have decreased expression of CD14 (similar to immature monocytic cells), this monocytic subset represents an activated monocytic population and should not be confused with immature monocytic cells. Non-classical monocytes differ from immature monocytic cells as this subtype expresses CD16 with altered intensity of typical monocytic markers. Decreased CD64 intensity is common on this subset (see Figure 1 E, F). Intermediate and non-classical monocytes may be relatively decreased in CMML (Selimoglu-Buet et al. 2015) as compared to reactive monocytosis. In CMML, classical monocytes characteristically account for the majority of the circulating monocytic cells. By contrast, in some inflammatory conditions (for instance sepsis), non-classical monocytes will be relatively increased.
Figure 1: Normal monocytic maturation in the marrow:
The upper row of dot plots shows granulocytic and monocytic cells from a normal marrow specimen while the lower row of dot plots shows only monocytic cells. Granulocytic cells ranging from promyelocytes to mature neutrophils are shown in green while monocytic cells are shown in pink. The black arrows present highlight changes in antigen expression seen on monocytic cells with maturation. A-D) Monocytic cells show high-level expression of CD33 and CD64 at all stages of maturation. Although intermediate levels of CD64 and CD33 may be seen on immature granulocytic precursors (promyelocytes in particular), the level of CD33 and CD64 is typically higher on monocytic cells. Normal maturing monocytic cells can express variable CD15, albeit usually at a lower level than on mature granulocytic cells. Immature monocytic cells express increased levels of HLA-DR with decreased CD13 and CD14. E,F) As compared to classical monocytes (pink arrow), which comprise the majority of monocytic cells, intermediate (blue arrow) and non-classical (red arrow) monocytes show increased expression of CD16 with decreased intensity expression of some monocytic markers including CD14 and CD64. Both populations are highlighted by the black ovals.
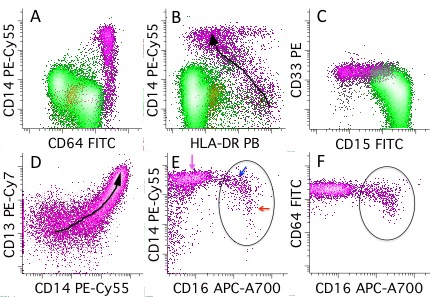
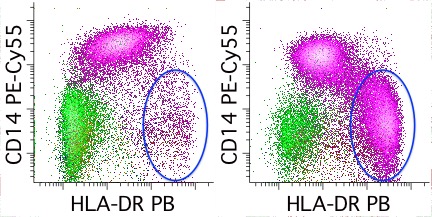
Figure 2: Neoplastic monocytic cells, peripheral blood versus marrow:
Data from concurrent peripheral blood (A) and marrow (B) specimens from a patient with acute myeloid leukemia (AML) with monocytic differentiation are shown. Both plots show all myelomonocytic cells with granulocytic cells shown in green and monocytic cells shown in pink. Both the blood and marrow show a relative increase in monocytic cells with an increase in CD14 low to negative immature monocytic precursors (blue oval); however, the proportion of immature monocytic cells in the marrow (33% of the white blood cells) is much higher than in the peripheral blood (3% of the white blood cells). Morphologic review of the marrow was diagnostic of AML with monocytic differentiation.
References:
Xu Y et al. Flow cytometric analysis of monocytes as a tool for distinguishing chronic myelomonocytic leukemia from reactive monocytosis. Am J Clin Pathol. 2005 Nov;124:799-806.
Yang DT et al. Flow cytometric analysis of different CD14 epitopes can help identify immature monocytic populations. Am J Clin Pathol. 2005 Nov;124:930-36.
Selimoglu-Buet et al. Characteristic repartition of monocyte subsets as a diagnostic signature of chronic myelomonocytic leukemia. Blood. 2015;125(23):3618-26.
Mukherjee et al. Non-classical monocytes display inflammatory features: Validation in Sepsis and Systemic Lupus Erythematous. Scientific Reports 5:13886 DOI:10.1038/srep13886.
Author: Sindhu Cherian