Ask an Expert
Back to Categories
How can flow cytometry identify normal and abnormal mast cells?
Mast cells are leukocytes of granulocytic (myeloid) derivation and reside predominately in extranodal and extra-medullary sites. Normally, mast cells are infrequent in the bone marrow (<1% of the marrow elements) although higher counts can be seen in the setting of autoimmune and allergic reactions which mast cells are thought to play a major role given the high histamine content of their granules.
Normal mast cells demonstrate a very characteristic immunophenotype with high CD117, intermediate CD33 (similar to monocytes), intermediate CD9 and CD71, low CD38 and CD11b, low-intermediate HLA-DR (less than monocytes and B cells but higher than T cells), without CD34 or CD19, and sit near the location of eosinophils (slightly higher CD45 than granulocytes) on normal plots of CD45/Side-scatter.
Aberrant expression of CD25, with or without CD2, is considered a minor criterion for the diagnosis of systemic mastocytosis according to the 2016 WHO classification of hematopoietic and lymphoid neoplasms and by itself should not be considered evidence of a neoplastic mast cell process. This aberrant immunophenotype can be seen in the post chemotherapy setting (see Cherian et al.) and therefore these findings should be taken with caution without the characteristic morphologic, molecular, and clinical manifestations of systemic mastocytosis.
Mast cells are typically under-represented by flow cytometry and therefore quantification is of little clinical utility. Given this under-representation, we recommend collecting a large number of events (~500,000 +) to ensure an adequate analytic sensitivity.
Given the significant granularity of these cells, autofluorescence of mast cells can complicate assay design especially on channels excited by violet (405 nm) and blue (488 nm) lasers (FITC predominantly). Nevertheless, a gating strategy based on high expression of CD117 is usually successful if erythroid precursors are fully lysed as there are almost no other cells with such high expression of CD117. Indeed, the high expression of CD117 should be considered when designing a panel for mastocytosis as spillover effects may limit the low level sensitivity for the aberrantly expressed markers of interest.
Example:
Examples of bone marrow samples with normal and abnormal mast cells are illustrated in the following flow cytometry dot-plots:
1- Bone marrow sample (normal mast cells in green and lymphocytes, B and T cells, in blue)

2- Bone marrow sample (normal mast cells in green)

3- Bone marrow sample (CD25+ abnormal mast cells in green)

4- Bone marrow sample (CD2+ and CD25+ abnormal mast cells in green)
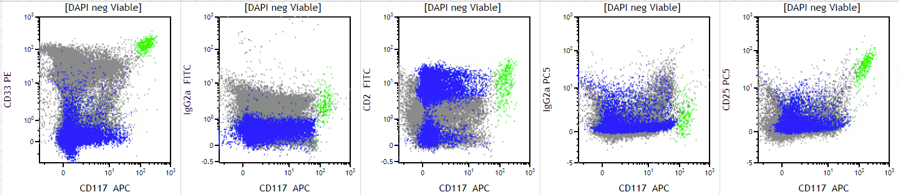
5- Bone marrow sample with KIT D816V mutation (CD2+ and CD25+ abnormal mast cells in green)

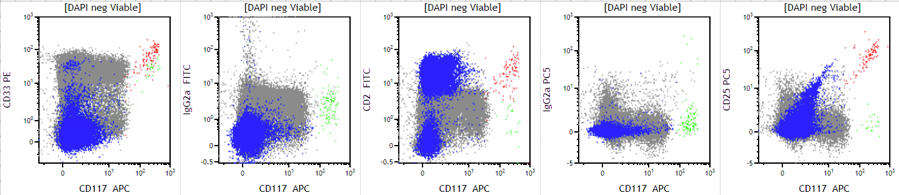
6- Bone marrow sample with both normal (green) and abnormal (red) mast cell populations
REFERENCES
1. Horny HP et al. Mastocytosis. 2016 WHO classification of hematopoietic and lymphoid neoplasms. IARC Press 2017 pp. 62-9
2. Cherian S et al. Expression of CD2 and CD25 on mast cell populations can be seen outside the setting of systemic mastocytosis. Cytometry B Clin Cytom. 2016 Jul;90(4):387-92.
Author: David P. Ng